A risk prediction model using multimodality ultrasound bests TI-RADS when it comes to evaluating thyroid nodules -- and could help avoid unnecessary biopsies, according to a study published June 27 in Radiology.
Researchers led by Fan Xiao from Fifth Medical Center of Chinese PLA General Hospital in Beijing found that their model, which incorporates sonographic features from conventional ultrasound, strain elastography, and contrast-enhanced ultrasound (CEUS), outperformed standard TI-RADS.
"By integrating the acoustic characteristics, morphologic structure, composition, textures, perfusion, and hemodynamic information of thyroid nodules, we hypothesized that multimodality ultrasound might allow for better risk stratification of thyroid nodules," Xiao and colleagues wrote.
Current guidelines from the American College of Radiology's TI-RADS risk model recommend using conventional ultrasound to assess risk in thyroid nodules. However, the researchers pointed out that fine-needle aspiration is often recommended for benign nodules, which may not be necessary. This is because of the high rates of false-positive findings, leading to what the researchers called "unsatisfactory" accuracy.
Previous studies have explored the potential of multiple ultrasonic methods in thyroid imaging, including elastography and CEUS. Xiao's team sought to test models they developed, which incorporate features from these modalities as well as conventional ultrasound for determining whether fine-needle aspiration is needed for suspicious thyroid nodules. From there, the group compared recommendation results with the TI-RADS model.
The study included data from 434 consecutive patients from nine hospitals who presented with a total of 434 thyroid nodules between 2020 and 2021. Of these, 259 nodules were determined to be malignant.
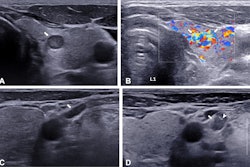
 (A) Imaging shows conventional ultrasound in a 49-year-old female participant with a thyroid nodule (white arrows) detected on a previous ultrasound image two weeks prior. The nodule is solid, hypoechoic, and taller than wide with the punctate echogenic foci (yellow arrow) and lobulated margin in the right lobe. The maximum diameter is 10 mm. The American College of Radiology TI-RADS system is TR5 level. The proportion of cystic component is 0%. (B) The elastogram shows blue to indicate stiffness (arrows in transverse cross-section) in the nodule. (C) The CEUS image (nine seconds, the start of the wash-in period of the thyroid nodule) shows early-phase hypoenhancement intensity (arrows on transverse cross-section) with slow-infusion wash-in mode. (D) CEUS imaging (36 seconds, the end of the maximum enhancement and the start of the wash-out period in the thyroid parenchyma) shows heterogeneous enhancement uniformity (arrows on transverse cross-section). The whole CEUS shows low blood volume. Both the predicted value (0.9) according to the nomogram of the multimodaluty model and the management of TI-RADS recommended fine-needle aspiration to the thyroid nodule. The final pathologic diagnosis was papillary thyroid carcinoma, and the participant underwent microwave ablation to the thyroid nodule. Images and caption courtesy of RSNA.
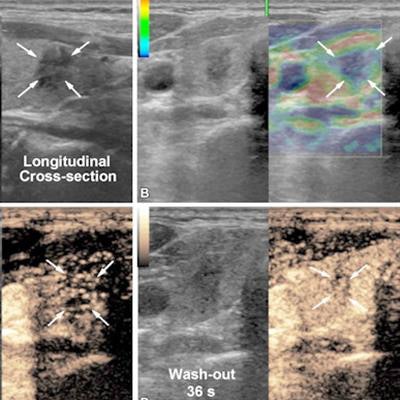
(A) Imaging shows conventional ultrasound in a 49-year-old female participant with a thyroid nodule (white arrows) detected on a previous ultrasound image two weeks prior. The nodule is solid, hypoechoic, and taller than wide with the punctate echogenic foci (yellow arrow) and lobulated margin in the right lobe. The maximum diameter is 10 mm. The American College of Radiology TI-RADS system is TR5 level. The proportion of cystic component is 0%. (B) The elastogram shows blue to indicate stiffness (arrows in transverse cross-section) in the nodule. (C) The CEUS image (nine seconds, the start of the wash-in period of the thyroid nodule) shows early-phase hypoenhancement intensity (arrows on transverse cross-section) with slow-infusion wash-in mode. (D) CEUS imaging (36 seconds, the end of the maximum enhancement and the start of the wash-out period in the thyroid parenchyma) shows heterogeneous enhancement uniformity (arrows on transverse cross-section). The whole CEUS shows low blood volume. Both the predicted value (0.9) according to the nomogram of the multimodaluty model and the management of TI-RADS recommended fine-needle aspiration to the thyroid nodule. The final pathologic diagnosis was papillary thyroid carcinoma, and the participant underwent microwave ablation to the thyroid nodule. Images and caption courtesy of RSNA.The team employed four multivariable models which incorporated patient age with nodule features on ultrasound, elastography features, and CEUS features. It also combined these into one multimodality model.
The researchers found that the multimodality ultrasound model had the highest area under the receiving operating characteristic curve (AUC) when recommending fine-needle aspiration (0.85). The TI-RADS model achieved an AUC of 0.63 (p < 0.001).
The group also found that at the 50% risk threshold, 31% of fine-needle aspiration procedures could be avoided with the multimodality ultrasound model, more than double that of TI-RADS at 15% (p < 0.001).
"In our study sample, 136 of 434 participants would not have undergone fine-needle aspiration, whereas malignant thyroid nodules would have been missed in 12 of 136 participants," the study authors wrote.
The researchers did report that they could not determine whether elastography or CEUS were superior to one another, as neither achieved statistically significant differences. In light of these results, they called for future research to explore which patients might benefit from elastography or CEUS rather than multimodal ultrasound.
The study can be found here.