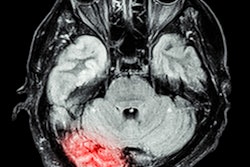
Patients with COVID-19 who present with acute neurologic symptoms may be at risk for large-vessel occlusion (LVO) stroke, and thus need prompt workup, according to an article published in the American Journal of Roentgenology (AJR).
The retrospective case-control study included patients who had a stroke code activated from March 16 to April 30 at a single system of six hospitals in the New York City boroughs of Manhattan, Queens, and Brooklyn. Demographic data, COVID-19 status, stroke-related risk factors, as well as clinical and imaging findings pertaining to stroke, were collected from electronic medical records (AJR, July 29, 2020).
"To our knowledge, this is the first study to describe an association between COVID-19 and large vessel strokes," wrote lead investigator Dr. Shingo Kihira from the Icahn School of Medicine at Mount Sinai.
In the 329 patients, 35.3% (116) had acute ischemic stroke confirmed with imaging; 21.6% (71) had LVO stroke; and 14.6% (48) had small-vessel occlusion (SVO) stroke. The most common LVO was middle cerebral artery segment M1-M2 occlusion. However, multifocal LVOs were observed in only 9.9% of patients with LVO stroke.
COVID-19 was present in 38.3% of patients. LVO stroke was present in 31.7% of patients with COVID-19, compared with 15.3% of patients without COVID-19. SVO stroke was present in 15.9% of patients with COVID-19 and 13.8% of patients without COVID-19.
The researchers found the presence of COVID-19 had a significant independent association with LVO stroke (odds ratio, 2.4) compared with absence of COVID-19. Also, after stratifying for race and ethnicity, the study results indicate the risk of large vessel stroke among patients with COVID-19 was 2.4 times as high as that among patients without COVID-19.