LOS ANGELES -- Two key biomarkers predict response to iodine-131 therapy in obese patients with differentiated thyroid cancer (DTC), according to research shared June 1 at the Society of Nuclear Medicine and Molecular Imaging (SNMMI) meeting.
The findings suggest that "obesity-related metabolic factors, particularly stimulated thyroglobulin and serum triglyceride levels, are independently associated with the therapeutic response to iodine-131 therapy in obese patients with differentiated thyroid carcinoma," said Yan Zhou of Huazhong University of Science and Technology in China. Zhou delivered her presentation virtually.
Thyroid cancer is a common endocrine disease, and its incidence has been steadily increasing around the world, she noted. DTC is a prevalent histological subtype of this cancer and tends to be associated with a favorable prognosis. But obesity increases risk of poorer outcomes in patients with the condition, she said, explaining that "obesity-related metabolic disturbances, chronic low-grade inflammation, and alterations in immune function may adversely influence tumor progression and treatment response."
The use of iodine-131 (I-131) therapy is common in the management of DTC after surgery, according to Zhou: it plays a key role in destroying any remaining thyroid tissue and treating metastatic disease. Yet research regarding the impact of obesity-related clinical, pathological, and metabolic characteristics to I-131 therapy in patients with DTC remains limited.
To address the knowledge gap, Zhou's team explored any associations between clinical, pathological, and metabolic factors in obese patients with DTC and response to I-131 therapy, "with the goal of improving risk stratification and optimizing individualized treatment strategies," she said.
The group conducted a study that included 457 obese patients with DTC and a body mass index (BMI) equal to or greater than 28.0 kg/m² who underwent iodine-131 therapy at Union Hospital at Tongji Medical College between January 2020 and December 2023. Average participant age was 40 years, and median follow-up time was 36 months. The researchers tracked clinical data such as sex, age at diagnosis, BMI, maximum tumor diameter, tumor multifocality, extrathyroidal extension, extranodal extension, tumor stage, lymph node stage, and metabolic factors (i.e., thyroid function, lipid metabolism, and liver function indicators). They categorized patients into two groups: "excellent response" (n = 269) and "not excellent response" (n = 188) using two established thyroid cancer assessment guidelines.
The team found that stimulated thyroglobulin (sTg) and serum triglyceride levels in particular independently predicted I-131 therapy outcomes. The group reported that the optimal cutoff value for triglycerides was 1.1 mmol/L (sensitivity, 86.5%; specificity, 26.7%, with an area under the curve [AUC] of 0.58), while the optimal cutoff value for sTg was 6.8 µg/L (sensitivity, 67.3%; specificity, 90%, with an AUC of 0.87).
Odds ratios for I-131 treatment outcomes according to biomarkers in obese patients with DTA | |||
Measure | Poor response | Excellent response | P-value |
| sTg (ug/L) | 65.4 | 3.44 | <0.001 |
| Triglycerides (mmol/L) | 1.96 | 1.71 | 0.020 |
| High-density lipoprotein cholesterol (mmol/L) | 1.04 | 1.1 | 0.002 |
Zhou and colleagues found that variables such as tumor or lymph node stage, high-density lipoprotein cholesterol, maximum tumor diameter, anti-thyroglobulin antibody (ATg), and iodine-131 dose did not show statistical significance for predicting I-131 treatment outcomes after surgery among obese DTC patients.
The findings "suggest that metabolic status should be considered in risk stratification and post-therapy evaluation of obese DTC patients," Zhou concluded.
Check out AuntMinnie’s full coverage of SNMMI 2026 on our ShowCast.






![RET-targeted PET tracer highlights neuroendocrine prostate cancer tumors. Representative PET imaging shows strong tumor uptake of the RET-binding peptide tracer [⁶⁸Ga]Ga-DOTA-RET-L7 in a neuroendocrine prostate cancer (NEPC) model, supporting highly specific, high-contrast detection.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/05/screenshot-2026-05-27-205827.278Ys6PYU3.png?auto=format%2Ccompress&fit=crop&h=167&q=70&w=250)




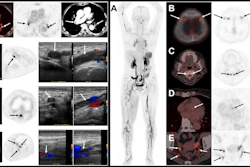
![(A-C) Representative whole-body maximum-intensity projection images and regional fused PET/CT images from three histologically confirmed osteosarcoma patients who underwent paired [68Ga]Ga-B7-H3-BCH PET/CT and 18F-FDGE PET/CT within seven days. (D) Multimodal imaging evaluation of Patient Three, including x-ray, MRI (T2-weighted imaging, T2WI), CT, and B7-H3 PET/CT.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/05/mei.XUQJWkpAJI.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)


![RET-targeted PET tracer highlights neuroendocrine prostate cancer tumors. Representative PET imaging shows strong tumor uptake of the RET-binding peptide tracer [⁶⁸Ga]Ga-DOTA-RET-L7 in a neuroendocrine prostate cancer (NEPC) model, supporting highly specific, high-contrast detection.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/05/screenshot-2026-05-27-205827.278Ys6PYU3.png?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)



