Paraganglioma:
Clinical:
Thoracic paragangliomas (also referred to as chemodectomas) are rare tumors- they account for less than 0.5% of mediastinal tumors and 1-2% of all paragangliomas [4]. They arise from chromaffin cells in paraganglia tissue in the paravertebral sympathetic chain, along the aorta, the A-P window, or the vagus nerve. Paragangliomas are more common in the abdomen than in the thorax. Men and women are affected equally (although vagal paragangliomas have a female predominance [4]). Patients usually present in the 4th to 5th decade of life [4]. The lesion may be associated with MEN syndromes or von Hippel-Lindau disease [4]. Most lesions are benign (and non-functioning) and surgical resection is curative. Only 10% of lesions behave aggressively and are typically locally invasive. Less than 2% are malignant [2], although the rate of malignancy is greater for thoracic paragangliomas than those occurring at other sites [4]. It is extremely uncommon for patients with mediastinal paragangliomas to have symptoms secondary to catecholamine secretion by the lesion (ie: extra-adrenal pheochromocytoma).X-ray:
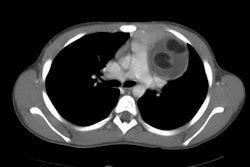
On CT the lesion is usually a sharply marginated, homogeneous soft tissue mass which demonstrates diffuse intense enhancement, reflecting its very vascular nature. It is commonly located in a para-aortic or para-spinous location. Lesions may occur in other sites, however, as paraganglia tissue is also found in the aorto-pulmonary window, along the recurrent laryngeal nerve, and near the proximal aspect of the subclavian arteries. Extensive cystic degeneration or hemorrhage can result in areas of low attenuation.On MRI the lesions have heterogeneous signal intensity with areas of signal void due to flowing blood on T1-weighted images (when large, the mass may have a salt-and-pepper appearance from vessel signal flow voids interspersed with hyperintense foci [4]). The lesion is of high signal on T2 images.
FDG PET shows mderate sensitivity for thoracic paragangliomas [4]. MIBG-positive tumors are more likely to be functional [4].
REFERENCES:
(1) RadioGraphics 1998; Ros PR, et al. Image interpretation session: 1997. 18: 195-228 (Case 6- 211-213) (No abstract available)
(2) Radiol Clin N Am 2005; Franco A, et al. Imaging evaluation of pediatric mediastinal masses. 43: 325-353
(3) AJR 2007; Balcombe J, et al. Cross-sectional imaging of
paragangliomas of the aortic body and other thoracic branchiomeric
paraganglia. 188: 1054-1058
(4) AJR 2016; Pavlus JD, et al. Imaging of thoracic neurogenic tumors. 207: 552-561