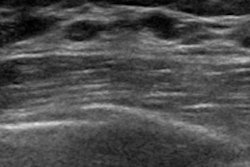
Nine unique patient and ultrasound features may enable breast imagers to distinguish benign from malignant complex cystic or solid breast lesions, according to research published on February 24 in Ultrasound in Medicine and Biology.
Lesion type, size, orientation, and vascularity were just a few of the features that were found through handheld ultrasound scans and linked to breast cancer. The combination of all nine factors resulted in a sensitivity of 77% and specificity of 82%, the authors reported.
"In addition to identifying whether a lesion is cystic or solid, [handheld ultrasound] is widely applied to tumor diagnosis, biopsy guidance, and even further treatment," wrote the authors, led by Dr. Huiling Xiang from the department of ultrasound at the Sun Yat-sen University Cancer Center in Guangzhou, China. "However, studies related to the diagnostic yield of [handheld ultrasound] in distinguishing benign from malignant complex cystic and solid breast lesions are limited."
The authors defined complex cystic lesions as those that are oval or round in shape with circumscribed margins but also have debris with low-level echoes. These lesions are common in middle-aged women and are often benign, but they do carry a nontrivial risk of malignancy. The researchers therefore wondered whether features on handheld ultrasound might be better able to differentiate complex cystic lesions that needed biopsy and ones that were likely benign.
To find out, the authors used data from 453 patients with 472 complex cystic and solid breast lesions who visited a university cancer center between 2000 and 2018. Radiologists with at least three years of breast imaging experience examined the lesions using handheld ultrasound with a high-frequency linear array transducer.
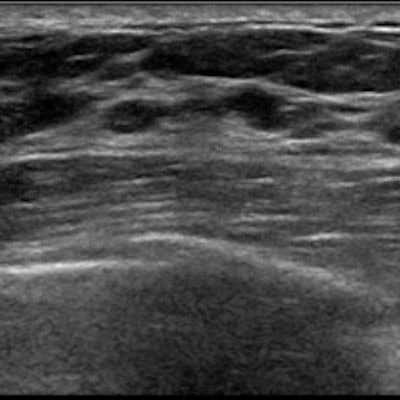
They also subdivided the lesions into four categories:
- Type I: Thick wall and/or septations, > 0.5 mm
- Type II: One or more mural or papillary nodules
- Type III: Mixed lesion that is more than 50% cystic
- Type IV: Mixed lesion that is more than 50% solid
The study included a variety of lesion types. About 13% of the lesions were classified as type I, 10% were type II, 21% were type III, and 55% were type IV.
Following biopsy, a little more than half of the lesions were confirmed as benign, while the remaining 45% were deemed malignant. However, the results varied based on lesion type.
The positive predictive value was significantly higher for type III or IV lesions than type I or II lesions. Other factors independently associated with malignancy included the following:
- Lesion diameter of more than 18 mm
- Lesion with irregular shape
- No parallel orientation
- Uncircumscribed margin
- Calcification
- Vascularity in the tumor
- Abnormal axillary lymph nodes
- Patient age of 52 or older
A lesion type of III or IV and a lesion diameter of more than 18 mm had the highest sensitivity (87%) and negative predictive value (82%) of any of the factors significantly associated with malignancy. Abnormal findings in axillary lymph nodes had the highest specificity (94%) and positive predictive value (83%).
It is important to note that even type I and type II lesions, which were not linked to malignancy in the study, still met the 2% malignancy threshold to qualify for a BI-RADS 4 categorization and biopsy. While the authors couldn't rule out any lesions as benign, they were able to better categorize them.
"Type I, II, and IV lesions can be assessed as BI-RADS 4B, while type III lesions can directly go into BI-RADS 4C, which allows a more accurate subclassification of complex cystic and solid breast lesions in clinical practice," the authors wrote.
In addition, the researchers excluded complicated cystic lesions without solid components and only included patients who had already undergone handheld ultrasound. As a result, the study may have selection bias.
Nevertheless, the findings reaffirm the power of handheld ultrasound as a powerful, secondary screening tool, the authors noted.
"Therefore, we may safely conclude that the [handheld ultrasound] is a useful modality in differential diagnosis of benign and malignant complex cystic and solid breast lesions and a tool complementing [mammography] in lesion detection," they wrote.