Cardiac imaging is at the proverbial heart of precision medicine, according to a talk delivered on March 6 at ECR 2026 in Vienna.
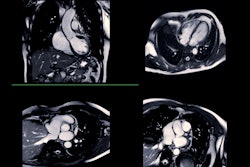
It requires the expertise of a range of imaging professionals and includes a variety of imaging exams, from coronary CT angiography (CCTA) and invasive coronary angiography to cardiac MRI and SPECT, presenter Michelle Williams, PhD, of the University of Edinburgh, told session attendees.
 Prof. Michelle Williams, PhD.ECR
Prof. Michelle Williams, PhD.ECR
"Cardiac imaging allows us to see valves, ventricles, the pulmonary and coronary arteries, the aorta, the pericardium, the atria, and pulmonary veins," she explained. "It contributes to precision medicine in cardiovascular care, [characterizing] stable or acute symptoms, offering screening, changing disease management, and improving outcomes."
The heart beats 2.5 billion times in a person's lifetime and "never has a day off," Williams noted.
"It's a mechanical system that we have never managed to replicate, even in this era of AI," she said. "So the first reason it is at the center of precision medicine is because it's an incredible organ."
Unfortunately, cardiovascular disease is a significant health problem around the world, with more than 620 million people affected, she said. It kills 20.5 million individuals per year. In fact, every three minutes someone dies from heart or circulatory disease, according to Williams.
"So as imagers, there [are lots of conditions we can assess] in the heart … and we really have an amazing armament of imaging tests that can be used, both invasive and noninvasive," she said. "We want to do the right test for the right patient at the right time."
Precision medicine in the cardiovascular sphere is about individualizing the diagnosis, according to Williams.
"If you don't have the right diagnosis, you can't have the right treatment," she said. "So diagnosis is absolutely central to [patient health] here, even more so today than it ever has been before."
Although there aren't yet protocols for screening for coronary artery disease, they could be coming, Williams noted.
"We do lung cancer screening," she said. "At some point in the next two to five years, do we need to think about upscaling our workforce to do cardiovascular screening as well? Ultimately, this is all about how we can change things for patients. Can we improve management and can we improve outcomes?"
Cardiac imaging use has increased as guidelines have been introduced, particularly CCTA and cardiac MRI, Williams noted. The nature of cardiac imaging has also changed, with noninvasive tests being used to determine whether more invasive studies are needed.
She described the benefits of cardiac MRI, noting that it provides a "wealth of information," but also highlighted the benefits of nuclear medicine, both SPECT and PET. For example, PET can help assess perfusion as well as metabolic pathways.
Fundamental to cardiac imaging is the multidisciplinary team -- radiographers, radiologists, nuclear medicine experts, cardiologists, nurses, and general practitioners.
"No one of us can do this on our own," she said. "We all need to work together."
Our full coverage of ECR 2026 can be found here.