Radiographics 1997 Mar;17(2):377-390. Cigarette smoking: CT and pathologic findings of associated pulmonary diseases.
Hartman TE, Tazelaar HD, Swensen SJ, Muller NL
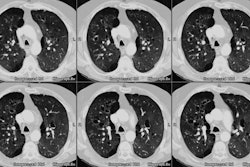
The health risks associated with cigarette smoking are well known. Cigarette smoking is the most important causative factor in the development of bronchogenic carcinoma. Pulmonary diseases such as chronic bronchitis, centrilobular and panacinar emphysema, respiratory bronchiolitis-associated interstitial lung disease (RB-ILD), and pulmonary Langerhans cell histiocytosis are also related to cigarette smoking. In adenocarcinoma and squamous cell carcinoma, the most common manifestation at computed tomography (CT) is a solitary pulmonary nodule; in small cell carcinoma, hilar and mediastinal adenopathy secondary to metastases; and in large cell carcinoma, a mass with central necrosis or cavitation in the lung periphery. For chronic bronchitis, the most common CT finding is bronchial wall thickening, but this finding is nonspecific. Emphysema, both centrilobular and panacinar associated with alpha-1-antitrypsin deficiency, usually manifests as areas of decreased attenuation and may involve bullous changes. However, centrilobular emphysema more commonly involves the upper lungs, whereas panacinar emphysema more commonly involves the lower lungs. Most patients with RB-ILD have normal high-resolution CT scans; however, abnormalities may be present, the most common of which are areas of ground-glass attenuation. CT appearance of pulmonary Langerhans cell histiocytosis varies depending on the disease stage: In the early stage, typical CT findings include multiple nodules, usually accompanied by cystic spaces with thin, well-defined walls. As the disease progresses, the cystic spaces become more numerous and the number of nodules decreases.
PMID: 9084079, MUID: 97237611