Toshiba America Medical Systems has formally launched U.S. sales of its Aquilion 16, the company’s 16-slice CT scanner. The system features a 40-row quantum detector, isotropic scanning capabilities, and enhanced image-reconstruction technology.
The Tustin, CA-based company said the scanner’s 40-row detector is capable of producing 16 simultaneous slices of 0.5 mm, 1 mm, or 2 mm with each gantry revolution, for a total z-axis coverage of 32 mm. In addition, the system accommodates scanning of larger patients with the capability to tilt 30 degrees, as well as a new couch with a scan range of 180 cm to accommodate taller patients.
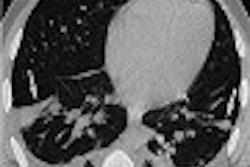
The vendor is also touting Aquilion’s ability to acquire isotropic volume data sets of any region of the body in a single breathhold. Traditional CT angiograms that usually take 60 seconds now require only 15 seconds with Aquilion, according to the manufacturer.
By AuntMinnie.com staff writersSeptember 26, 2002
Related Reading
Toshiba’s Aquilion 16 CT scanner receives FDA clearance, July 18, 2002
Toshiba taps sales VP, June 20, 2002
Toshiba hires LaPoint, June 19, 2002
Toshiba scores another VA contract, June 4, 2002
Toshiba lands VA contract, June 3, 2002
Copyright © 2002 AuntMinnie.com