
Tuesday, November 30 | 10:50 a.m.-11:00 a.m. | SSG07-03 | Room S102D
Boosting the equipment utilization rate to 75% in 2011 as a way to lower Medicare costs will actually limit resources as a flood of new enrollees enter the system, especially in rural areas, according to researchers from St. Luke's-Roosevelt Hospital Center in New York City.In this Tuesday morning session, Amit Sura, MD, and colleagues plan to present findings from a literature review they conducted to evaluate whether focusing on equipment utilization is the best way to cut costs, versus focusing on other measures such as appropriateness criteria and preauthorization.
From the literature, the team found that from 2005 on, the rate of procedure volume has decreased, averaging growth of 1.2% over three years compared to 5.6% from 2000 to 2005. In the studies, 117 imaging centers were asked how their practices would change if the rate was unable to be met and reimbursement fell by 50%: Sura's team found that 29% of these centers would drop Medicare, 41% would limit access to Medicare beneficiaries, and 46% would close.
A rate of 75% is not feasible when the rate of studies conducted has decreased, Sura's group concluded, and high rates will force rural imaging centers to deny Medicare patients vital tests. Instead, the group suggested, developing and enforcing national standards helps curb the overutilization of studies, without requiring centers to meet unfeasible fixed utilization rates for equipment they own.
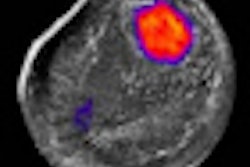
![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&fit=crop&h=100&q=70&w=100)






![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)










