A study found that incorrect AI suggestions significantly impact radiologist performance in mammography, with false-negative AI prompts causing reader sensitivity to drop by 32 percentage points and reducing visual attention to cancer cases. The research highlights the importance of optimizing AI thresholds and minimizing false-negative suggestions to prevent automation bias in breast cancer screening.
- 32-point sensitivity drop: Median reader sensitivity fell from 71% to 39% when AI provided false-negative suggestions in mammography interpretation.
- Automation bias confirmed: Radiologists showed reduced fixation rates and shorter gaze duration when reviewing cases with false-negative AI prompts, indicating decreased visual scrutiny.
- Read time impact: Cases with four or more AI prompts took 34 seconds to interpret versus 25 seconds with no prompts, potentially compromising workflow efficiency.
- Training implications: Experts emphasize the need for radiologist education on automation bias risks and critical evaluation of AI recommendations in daily clinical practice.
Incorrect AI suggestions may influence reader accuracy and visual search behaviors when reading mammograms, according to findings published July 14 in Radiology.
False-negative AI suggestions led to median reader sensitivity dropping by 32 percentage points, as well as reduced fixation rates, wrote a team led by Yan Chen, PhD, from the University of Nottingham in England.
“These findings highlight the importance of carefully optimizing AI thresholds and prompt accuracy to mitigate automation bias and effectively integrate AI into screening mammography workflows,” the Chen team wrote.
Automation bias is a persistent concern among radiologists who use AI. However, the researchers noted that only limited research has been done to measure changes in reader diagnostic accuracy in AI-assisted interpretation of medical images.
Chen and colleagues in their pilot study explored how incorrect AI suggestions influence the diagnostic accuracy, read times, and visual search behavior of radiologists who interpret screening mammograms.
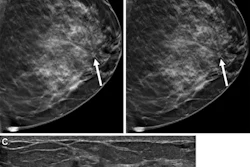
![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&dpr=2&fit=max&q=70&w=700) A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.RSNA
A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.RSNA
For the study, 10 mammography readers interpreted cases with and without AI in multiple rounds. In the first round, the readers interpreted cases without AI. In round two, conducted six weeks later, they used a commercially available AI tool as a decision support. The tool displayed prompts with a region score of 10 or higher (scale, 0 to 100). Eye-tracking cameras recorded maintained gaze over specific image areas.
Final analysis included a test set of 60 cases, including 26 true-positive, 14 false-negative, 14 false-positive, and six true-negative AI suggestions.
The researchers reported the following findings:
Median reader sensitivity dropped in cases with false-negative AI suggestions when reading cases with AI (39%) compared with unassisted reading (71%, p = 0.002).
Reader specificity rose for cases with false-positive AI suggestions (39% vs. 21%; p = 0.004).
A greater number of visible (true-positive and false-positive) AI prompts led to longer median read times, from 25 seconds (zero prompts) to 34 seconds (four or more prompts; p = 0.001).
Readers fixated less when reviewing cancer cases that AI failed to detect (false-negative suggestions) compared with unassisted reading (0.44 vs 0.47 fixations per second; p = 0.03).
Readers had shorter fixation durations when interpreting cases with false-negative AI suggestions compared with unassisted reading (0.54 vs. 0.56 seconds; p = 0.001).
“These findings are consistent with behaviors associated with automation bias when using AI,” the study authors wrote.
They added that their results “should be interpreted with consideration” and used to inform the design of future studies.
“Yet, these findings suggest that vendors prioritize AI algorithms and recall thresholds to minimize false-negative suggestions, as human readers may dismiss false-positive suggestions,” the authors wrote. “Changes should not increase the number of prompts, which was associated with longer read times, potentially compromising efficiency.”
Two accompanying editorials highlighted potential implications and ideas for future studies. Paola Clauser, MD, PhD, from the Medical University of Vienna wrote that future studies should focus on understanding the mechanisms of automation bias in radiology readings, on increasing the awareness of radiologists on this issue, and on supporting a critical approach in the daily use of AI.
“In addition, particular care should be taken in preparing residents and young radiologists and in studying the risks and drawbacks associated with automation bias in the learning process,” Clauser wrote.
And evaluating AI in medical imaging must evolve from algorithms alone to complete diagnostic systems, according to another editorial written by Nooshin Abbasi, MD, and Catherine Giess, MD, both from Brigham and Women’s Hospital and Harvard Medical School in Boston.
“As AI systems continue to evolve and radiologists gain greater experience using these tools, future studies across diverse clinical environments will be important to understand how human-AI interactions change during real-world deployment,” they wrote.
Read the full study here.