Collateral blood vessel status measured by CT angiography was associated with 90-day functional outcomes in patients with acute stroke due to medium-vessel occlusion (MeVO), according to a study published May 26 in Radiology.
The finding is from a post-hoc analysis of 529 participants in the in the Endovascular Treatment to Improve Outcomes for Medium Vessel Occlusions (ESCAPE-MeVO) trial, which tested whether endovascular thrombectomy (EVT) could improve outcomes for patients, noted lead author Johanna Ospel, MD, PhD, of the University of Calgary in Alberta, Canada, and colleagues.
“CT angiography-based collateral status was the imaging variable that was consistently associated with ordinal modified Rankin Scale score at 90 days," the group wrote.
The ESCAPE-MeVO trial included 530 patients from five countries and concluded in June 2024. The trial found no overall benefit of EVT plus usual care versus usual care alone in patients with acute MeVO stroke. However, because MeVO represents a heterogeneous patient population, Ospel and colleagues performed a post-hoc analysis to assess whether any baseline imaging characteristics could identify subgroups in whom reperfusion therapies might be beneficial or harmful.
The group assessed head CT, CT angiography (CTA), and CT perfusion baseline imaging characteristics, including occlusion site and collateral status. Outcomes stratified by those imaging characteristics were then compared between the EVT and control groups, with the primary outcome being the 90-day modified Rankin Scale (mRS) score, ranging from 0 (no disability) to 6 (death).
According to the analysis, most medium-vessel occlusions (442 of 522 [84.7%]) were in the middle cerebral artery territory. Collateral status at CTA was good in 129 of 517 participants (25.0%), moderate in 276 (53.4%), and poor in 111 (21.5%), the researchers reported.
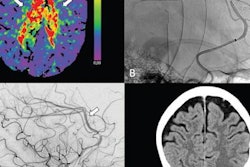
 Exemplary cases from the ESCAPE-MeVO trial illustrating good, moderate, and poor collateral status at baseline multiphase CT angiography (CTA). (A) Sagittal image shows a left anterior middle cerebral artery medium-vessel occlusion (MeVO) with a calcified thrombus (arrow). (B–D) Axial images show the (B) arterial, (C) peak venous, and (D) delayed venous phases of the baseline multiphase CTA examination. The affected brain parenchyma is highlighted by the dashed outline. The collateral status is good, with early filling of more than 50% of the leptomeningeal collaterals compared with the contralateral side in the arterial phase (B), and there is no delayed washout in the peak venous (C) or delayed venous phase (D). (E) Sagittal image shows a left anterior middle cerebral artery MeVO (arrow). (F–H) Axial images show the (F) arterial, (G) peak venous, and (H) delayed venous phases of the baseline multiphase CTA examination. The affected brain parenchyma is highlighted by the dashed outline. The collateral status is moderate (more than 25% but less than 50% filling of the leptomeningeal collaterals in the affected territory compared with the contralateral side) on the arterial (F) and peak venous (G) phase, and there is delayed washout in the late venous phase (H). (I) Sagittal image shows a posterior dominant middle cerebral artery MeVO (arrow). (J–L) Axial images show the (J) arterial, (K) peak venous, and (L) delayed venous phases of the baseline multiphase CTA examination. The affected brain parenchyma is highlighted by the dashed outline. The collateral status is poor, with almost no collateral filling.RSNA
Exemplary cases from the ESCAPE-MeVO trial illustrating good, moderate, and poor collateral status at baseline multiphase CT angiography (CTA). (A) Sagittal image shows a left anterior middle cerebral artery medium-vessel occlusion (MeVO) with a calcified thrombus (arrow). (B–D) Axial images show the (B) arterial, (C) peak venous, and (D) delayed venous phases of the baseline multiphase CTA examination. The affected brain parenchyma is highlighted by the dashed outline. The collateral status is good, with early filling of more than 50% of the leptomeningeal collaterals compared with the contralateral side in the arterial phase (B), and there is no delayed washout in the peak venous (C) or delayed venous phase (D). (E) Sagittal image shows a left anterior middle cerebral artery MeVO (arrow). (F–H) Axial images show the (F) arterial, (G) peak venous, and (H) delayed venous phases of the baseline multiphase CTA examination. The affected brain parenchyma is highlighted by the dashed outline. The collateral status is moderate (more than 25% but less than 50% filling of the leptomeningeal collaterals in the affected territory compared with the contralateral side) on the arterial (F) and peak venous (G) phase, and there is delayed washout in the late venous phase (H). (I) Sagittal image shows a posterior dominant middle cerebral artery MeVO (arrow). (J–L) Axial images show the (J) arterial, (K) peak venous, and (L) delayed venous phases of the baseline multiphase CTA examination. The affected brain parenchyma is highlighted by the dashed outline. The collateral status is poor, with almost no collateral filling.RSNA
Collateral status was the imaging variable associated with the primary outcome in the multivariable analysis (adjusted common odds ratio, 0.82). The probability of EVT achieving an adjusted mRS score of 0 or 1 was lower with EVT (25%) in participants with poor collaterals (vs 37% in the control arm) and higher in those with good collaterals (47% in the EVT arm vs 36% in the control arm), although the difference was not statistically significant, according to the findings.
“These findings have implications for future research to determine which patients with MeVOs benefit from EVT. Stringent patient selection based on CTA collateral status at baseline needs to be evaluated in a multicenter prospective study,” the group wrote.
In an accompanying editorial, Cem Bilgin, MD, and David Kallmes, MD, both of the Mayo Clinic in Rochester, MN, wrote that readers should interpret the study less as a verdict on MeVO thrombectomy than as a signal that future imaging-centered trials will need to move toward refining phenotyping of tissue risk and treatment responsiveness.
“We need to develop better collateral scoring in distal territories, perfusion thresholds tailored to smaller vascular beds, and structured descriptions of eloquent cortical risk,” they wrote.
The central message is not that MeVO thrombectomy should be abandoned, but that its routine use has not been supported in broad trial populations and that progress will depend on better imaging phenotyping and more refined patient selection for MeVO thrombectomy, Bilgin and Kallmes concluded.
The full study is available here.