The RSNA is launching a new database called the RSNA International COVID-19 Open Radiology Database (RICORD) to house a collection of anonymized COVID-19 medical images for research and clinical use.
The database will include not only images but also clinical information and expert annotation, and it will be available to research and education institutions around the world. The RSNA notes that 200 institutions have expressed interest in participating in the RICORD project.
The inspiration for RICORD was the rapidity with which scientists around the world isolated and sequenced the SARS-CoV-2 virus. The virus's sequenced genome was quickly made available to the global research community, according to the RSNA.
The RSNA has created data-sharing agreements with RICORD contributors, as well as tools to organize, deidentify, and transfer data to RICORD safely and conveniently. The database also connects to a storage infrastructure from the U.S. National Institutes of Health. What's more, researchers will be able to use tools like artificial intelligence and deep learning to analyze images in the database.
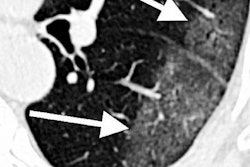
The first version of RICORD, v1.0, consists of an annotated core dataset of a subset of chest x-ray and CT exams in DICOM format with labels made by annotations from expert radiologists. The RSNA's COVID-19 AI Task Force over time will update and expand both the volume and variety of data available in RICORD, according to Dr. Matthew P. Lungren, chair of the task force.
More information is available on the RSNA's website.