Chest x-rays acquired when patients present in the emergency room (ER) with COVID-19 symptoms can predict the severity of the disease, particularly in young and middle-aged adults, according to a study published May 14 in Radiology.
The study findings demonstrate x-ray's value in helping physicians identify, triage, and treat high-risk patients, wrote a team led by Dr. Danielle Toussie of Mount Sinai Hospital in New York City.
"We demonstrate how valuable x-rays can be during this pandemic because, by evaluating disease in different portions of the lungs, we can predict outcomes, which can potentially help appropriately allocate resources and expedite treatment in the most severe cases," Toussie said in a statement released by the hospital.
The researchers developed an x-ray scoring system to evaluate COVID-19 disease severity in order to better determine which patients need to be hospitalized and/or intubated.
"We came up with the scoring system because we had clinicians asking us what we see on chest x-rays of COVID-19 patients," Toussie said. "We would tell them, 'We see this opacity here or that opacity there,' but then they would ask, 'What does that mean for my patient?' "
Toussie and colleagues evaluated records from 338 COVID-19 patients who were treated at three Mount Sinai locations in March. All underwent chest x-ray in the emergency room; of the total, 145 (43%) were admitted.
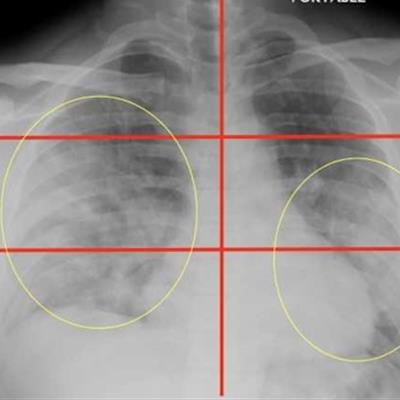
The team reviewed race and information on preexisting conditions on each patient, analyzed the x-rays for COVID-19 patterns, and divided them into six zones: upper right, upper left, middle right, middle left, lower right, and lower left. They then developed a scoring system from 0 to 6 to measure disease severity (lower severity scores, 0 to 2; higher scores, 3 to 6). Higher severity scores corresponded with lung involvement in multiple areas.
Overall, the researchers found the following:
- Patients with the highest scores were 6.2 times more likely to be hospitalized and 4.7 times more likely to be intubated.
- Men were more likely than women to have higher scores and be admitted to the hospital, but they were not more likely to be intubated.
- Obese patients were more likely to have higher scores and require hospital admission.
- The researchers found no significant differences in outcomes between patients of different races or ethnicities when they adjusted for age, gender, comorbidities, and weight.
| Chest x-ray severity score and percentage of patients intubated | |
| Severity score (number of patients) | Percentage of patients intubated |
| 0 (34) | 6% |
| 1 (15) | 7% |
| 2 (38) | 16% |
| 3 (14) | 14% |
| 4 (32) | 31% |
| 5 (7) | 43% |
| 6 (5) | 80% |
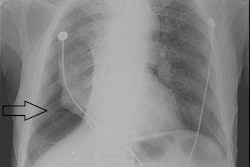
 Top image: Chest radiograph of a 23-year-old male with no past medical history who tested positive for COVID-19 via reverse transcription polymerase chain reaction (RT-PCR) and was subsequently discharged from the emergency department with home care and isolation precautions. Portable chest x-ray shows right and left peripheral lower lung zone hazy opacities; total score = 2. Bottom image: Chest radiograph in a 32-year-old overweight (BMI = 30) male positive for COVID-19 with a history of childhood asthma who was subsequently admitted and intubated in the intensive care unit for three days. Portable chest x-ray shows opacities in all three right lung zones and in the left middle and lower lung zones; total score = 5. Images courtesy of Mount Sinai Health System.
Top image: Chest radiograph of a 23-year-old male with no past medical history who tested positive for COVID-19 via reverse transcription polymerase chain reaction (RT-PCR) and was subsequently discharged from the emergency department with home care and isolation precautions. Portable chest x-ray shows right and left peripheral lower lung zone hazy opacities; total score = 2. Bottom image: Chest radiograph in a 32-year-old overweight (BMI = 30) male positive for COVID-19 with a history of childhood asthma who was subsequently admitted and intubated in the intensive care unit for three days. Portable chest x-ray shows opacities in all three right lung zones and in the left middle and lower lung zones; total score = 5. Images courtesy of Mount Sinai Health System.The study results highlight that COVID-19 findings on chest x-ray can help predict the disease's severity, said senior author Dr. Adam Bernheim in the statement.
"[Our work demonstrates] the role of radiology not only in diagnosis but also in predicting, triaging, and risk-stratifying COVID-19 patients so that those at highest risk for severe disease can be immediately identified from the moment of the very first chest x-ray upon presentation," he said.