PITTSBURGH – Molecular breast imaging (MBI) can help make breast imaging workflows more efficient, according to a presentation given April 12 at ARRS 2026.
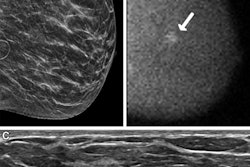
In her talk, Amy Conners, MD, from the Mayo Clinic in Rochester, MN, discussed how MBI visualizes cancers, especially those in dense breasts, and how radiologists should and should not use the technique.
“It’s a good technique for being able to see through dense breast tissue,” Conners told AuntMinnie.com. “We don’t recommend using it in a screening setting, but it’s a good adjunct to be able to screen patients.”
MBI has shown high performance in detecting breast cancers in women. It is superior to conventional mammography for imaging dense breasts.
Conners cited a 2025 analysis of the Density Molecular Breast Imaging and Tomosynthesis to Eliminate the Reservoir (MATTERS) Trial, which found that MBI detected an additional 6.7 cancers per 1,000 screenings one year after digital breast tomosynthesis (DBT) screening. MBI also found an additional 3.5 cancers per 1,000 screenings at the second year after DBT screening. And among the incremental cancers detected only by MBI, 70% were found to be invasive while 20% were node positive.
However, MBI use is relatively low in the U.S. compared to MRI. This may be due to concerns that women may have about the use of additional radiation for imaging their breasts. Competing imaging modalities such as breast MRI or contrast-enhanced mammography (CEM) may also push MBI’s use down, along with the need to invest in dedicated technology.
Conners said the “vast majority” of MBI indications are screening for dense breast tissue and that key learnings for establishing a care process model include the following: collaborate with referrers, emphasize work-up in symptomatic, and refer patients to MRI if they qualify.
“It [MBI] is a pretty accessible technique, so you don’t have to be an academic breast center to be successful with it,” she said.
For work-up of positive findings, Conners highlighted protocols from the Mayo Foundation for Medical Education and Research. After a positive MBI exam, a diagnostic mammogram and/or breast ultrasound exam are performed. Benign findings lead to screening being resumed, suspicious findings lead to guided biopsy, and no matching findings lead to MBI assessment. The latter includes a follow-up MBI exam at six months post-screening.
Conners added that her clinic considers women for MBI if they are ages 40 or older and have either category C or D breast density.
Amy Conners, MD, addresses the relatively low use of MBI in the U.S., as well as opportunities for growing the technique's presence.
Pros, cons, and limitations
Conners highlighted several advantages for using MBI. These include good supplemental yield, high likelihood of cancers being significant, good toleration by women, and short interpretation times, among others. Conners added that Tc-99m is widely available and considered safe for patients.
However, some drawbacks to MBI include less sensitivity compared to MRI, the need for an injection, vendor instability, the need to purchase a dedicated system, and the use of radiation. Conners also said that MBI-guided biopsies are not widely available.
For the radiation aspect, Conners noted that women absorb about 2 mSv when undergoing MBI, comparable to a head CT exam. Known carcinogenic effects are present around 100 mSv or higher, while annual background radiation exposure is less than 10 mSv.
“It [MBI dose] is more than a mammogram, but still quite low,” Conners said. “It allows us to have these conversations that … we can compare apples to apples. It’s nice to put it into a larger context.”
Conners also outlined several ways to not use MBI. These include imaging calcifications from ductal carcinoma in situ (DCIS), avoiding work-up of findings on mammography or ultrasound, avoiding biopsy of suspicious findings, and using MBI as a primary screening tool.
MBI also struggles with imaging axillary lymph nodes, low-grade findings, lobular histology, and findings 6 mm or smaller. It also has 1 cm less posterior tissue in the field of view compared to mammography.
Still, Conners said MBI represents a viable imaging option for women with dense breasts and that if criteria are followed, MBI can find many clinically significant cancers.












![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)



