Researchers from Massachusetts General Hospital (MGH) are using the novel approach of combining functional MRI (fMRI) and electroencephalography (EEG) to determine the level of consciousness in intensive care unit patients with severe traumatic brain injury (TBI), according to a study published online July 20 in Brain.
The strategy reportedly is the first attempt to use the two modalities collaboratively on acutely ill patients whose clinicians face critical decisions of how or whether to proceed with life-sustaining treatment.
"Early detection of consciousness and brain function in the intensive care unit [ICU] could allow families to make more informed decisions about the care of loved ones," said co-lead author Dr. Brian Edlow, from MGH's Center for Neurotechnology and Neurorecovery, in a release from the university. "Also, since early recovery of consciousness is associated with better long-term outcomes, these tests could help patients gain access to rehabilitative care once they are discharged from an ICU."
Costly errors
Previous research has suggested that as many as 40% of conscious patients are misclassified as unconscious. While fMRI or EEG can detect cases of more obvious consciousness among patients who have progressed to rehabilitation or nursing care facilities, no study has been conducted on seriously injured ICU patients.
The researchers enrolled 16 patients with severe traumatic brain injury at MGH's ICU. At the start of the study, eight patients could respond to language, three were classified as minimally conscious with no language response, three were classified as vegetative, and two were in a coma. The study also included 16 healthy age- and sex-matched volunteers who served as a control group.
Functional MRI scans were performed as soon as the subjects were stable enough for the procedure. When possible, EEG readings were taken within 24 hours after the fMRI scan.
The researchers also set up scenarios to test the subjects' abilities. For example, the subjects were asked to imagine squeezing and releasing their right hand while in the MRI scanner and while EEG readings were taken. This test is designed to detect a mismatch between their ability to imagine performing a task and their ability to physically express themselves, known as cognitive motor dissociation.
Through the exercise, the researchers detected evidence of covert consciousness in four (50%) of the eight patients who were unable to respond to language in the bedside exams, including the three classified as vegetative. Interestingly, approximately 25% of the healthy controls had no detectable brain response in the hand-squeeze imagery test.
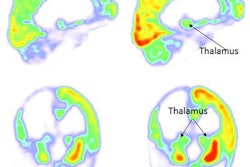
The subjects were also exposed to brief recordings of spoken language and music during both fMRI and EEG to detect activity in certain regions of the brain. In this test, higher-order cortex activity was seen in two additional subjects.
While higher-order cortical activity doesn't prove that a patient is conscious, finding a response in those structures could have implications for a patient's eventual recovery, Edlow said.
Results vs. outcome
In fact, no associations were found between early brain responses and long-term outcomes. The researchers suggested this could be due to the study's small cohort or the fact that several patients were sedated during the fMRI and EEG tests.
A negative response is not necessarily an indication that a patient has a low likelihood of recovery, Edlow added. In fact, one comatose patient who had no responses to language, music, or motor imagery in early fMRI and EEG tests proceeded to an excellent recovery six months later.
It's "difficult to measure the false-positive rate for stimulus-based fMRI and EEG tests in these patients, since there is no definitive, gold-standard test to diagnose their level of consciousness," he said. "Much more work needs to be done to determine the utility of these techniques for detecting consciousness in patients with severe traumatic brain injuries."
Indeed, the researchers plan to continue their work to improve the accuracy of these tests with a larger follow-up study in the near future.