A research group from Brigham and Women's Hospital in Boston has found that PET/CT fluoroscopy is feasible and has the potential to assist doctors performing PET/CT-guided tumor ablations.
A team led by Dr. Liwei Jiang tested a high-speed image fusion technique to generate and display PET/CT fluoroscopy images during PET/CT-guided tumor ablations in a group of cancer patients. The first-time use of the technique showed promise, the investigators noted.
"PET/CT fluoroscopy may facilitate targeting of radiotracer-avid masses with poor visibility on CT fluoroscopy images," the group wrote. The study was published May 2 in the Journal of Vascular and Interventional Radiology.
PET/CT is being increasingly used to guide tumor ablations because of its advantages in revealing tumors not conspicuous on other modalities, the authors explained. CT fluoroscopy is a safe and effective guidance tool, yet it is limited in detecting tumors with poor visibility -- for example, those obscured by metallic artifacts from interventional procedures.
In this study, the authors hypothesized that high-speed image fusion technology could be used to potentially overcome such obstacles by generating and displaying PET/CT fluoroscopy images during PET/CT-guided tumor ablations.
They used a multimodal image fusion platform (IGTFusion, IGI Medical Technologies) with proprietary software running on a dedicated workstation. The system received DICOM images pushed from the scanner, followed by near real-time image registration. The acquired PET dataset was fused to each CT fluoroscopy dataset as it arrived, and the fused images were displayed for physicians on an in-room monitor.
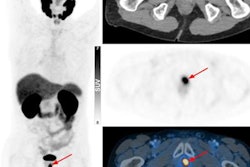
During 14 procedures, PET/CT fluoroscopy images were generated and displayed, with a mean of four PET/CT fluoroscopy acquisitions obtained per procedure. In three procedures treating four hepatic metastatic tumors, target visibility was poor on CT and CT fluoroscopy images alone. However, PET/CT and PET/CT fluoroscopy allowed for more confident targeting of the tumors, the researchers reported.
In addition, the mean lag time from CT fluoroscopy acquisition to the in-room display of the fused PET/CT fluoroscopy image was 21 seconds (plus or minus 8 seconds), with registration accuracy visually satisfactory in all but one procedure, the investigators reported.
"Conceptually, PET/CT fluoroscopy represents the extension of CT fluoroscopy to PET/CT for guiding interventional procedures of radiotracer-avid tumors," the group wrote.
While promising, the authors noted that this was a proof-of-concept study and not designed to demonstrate clinical outcomes, reductions in procedural time, or reductions in number of intraprocedural PET/CT acquisitions.
"These endpoints will be studied in the future," they concluded.