Sunday, November 27 | 1:30 p.m.-2:00 p.m. | S4-STCE-2 | Learning Center Theater
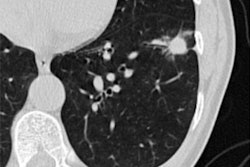
Photon-counting CT could be a useful tool for early diagnosis of interstitial lung disease -- although it does impart more radiation than conventional high-resolution CT, according to research results to be shared in a Sunday afternoon poster session.Interstitial lung disease is a dangerous condition in people with rheumatoid arthritis, noted a team led by presenter Dr. Nikolett Marton, PhD, of Semmelweis University in Budapest, Hungary. Early diagnosis -- and antifibrotic therapy -- can improve patient outcomes. Patients typically undergo high-resolution CT for this indication, but Marton's team sought to assess the efficacy of photon-counting detector CT for detecting lung parenchymal involvement in rheumatoid arthritis sufferers.
For their study, the investigators included 37 rheumatoid arthritis patients without a previous interstitial lung disease diagnosis. All underwent both high-resolution CT and photon-counting detector CT exams. Radiologist readers used a five-point scale to score the extent of lung abnormalities in each lung lobe, calculating a total disease score by the sum of these.
The group did find that photon-counting CT imparted more radiation compared to high-resolution CT (410 mGy-cm versus 27.6 mGy-cm). However, photon-counting CT was better at visualizing bronchiectasis and fibrosis, leading the researchers to the conclusion that "ultrahigh resolution photon-counting detector CT provides more detailed information regarding interstitial lung disease in patients with rheumatoid arthritis than high resolution photon-counting detector CT."