T1a: A tumor less than or equal to 2 cm in
greatest dimension that is completely surrounded by lung or visceral pleura,
without bronchoscopic evidence of
invasion more proximal than the lobar bronchus (i.e., not in the main bronchus)
T1b: A tumor larger than 2 cm and less than or equal to 3 cm in greatest
dimension, surrounded by lung or visceral pleura, without bronchoscopic evidence of
invasion more proximal than the lobar bronchus (i.e., not in the main bronchus)
Example 1: This is an example of a right lung T1a lesion
(in this case an adenocarcinoma). The tumor measures 2.4 cm in size and is completely
surrounded by lung.
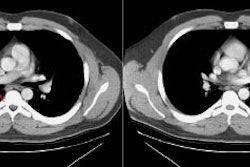
Example 2: This is an example of a T1a lesion in the left
lung (the nodular density in the right lung anteriorly [blue arrow] is the inferior margin
of the right clavicular head). The tumor measures 1.8 cm in size and is completely
surrounded by lung. A thin linear density radiates to the pleural surface from the lesion-
this is referred to as a "pleural tag" which is felt to represent tumor-induced
thickening of the interlobular septa. There is a focal triangular-shaped pleural-based
density identified at the insertion of the "pleural tag" (black arrow). This
finding is felt to be secondary to the desmoplastic reaction incited by the tumor. There
is retraction of the visceral pleura towards the lesion, and a small quantity of fluid
collects within the space formed between the visceral and parietal pleura producing the
finding identified on computed tomography. The finding does not indicate visceral pleural
invasion.
T2:
T2a: A tumor larger than 3 cm, but less than
or equal to 5 cm, surrounded by lung, or a tumor ≤ 5 cm that invades
visceral pleura, involves the main bronchus more than 2 cm from the carina
without collapse of the entire lung, or causes atelectasis or post
obstructive pneumonia not involving the entire lung. Visceral pleural
invasion has been defined as invasion extending through the elastic layer of
the viseral pleura to the surface of the viseral pleura- use of elastin
stains is recommended for determination of this feature.
T2b: A tumor larger
than 5 cm, but less than or equal to 7 cm, invades the visceral pleura,
involves the main bronchus more than 2 cm from the carina without collapse of
the entire lung, or causes atelectasis or post obstructive pneumonia not
involving the entire lung
i) Larger than 5 cm in largest dimension:
T2b
This large squamous cell carcinoma measures 5.4 cm in
transverse dimension. Linear densities radiate to the pleural surface from the lesion.
There is a focal pleural-based density identified laterally (blue arrow), but the
underlying subpleural fat is not disrupted. This finding is likely due to the desmoplastic
reaction incited by the tumor. As previously discussed, retraction of the visceral pleura
towards the lesion permits the development of a potential space between the visceral and
parietal pleura. A small quantity of fluid within the space can produce a soft-tissue
opacity between the lesion and the pleural surface.
ii) Lesion associated with atelectasis or post-obstructive
pneumonitis that extends to the hilar region, but does not involve the entire lung-
T2a
In this patient with squamous cell
carcinoma, there is a small endobronchial lesion at the origin of the left upper lobe bronchus (blue arrow). There is
left upper lobe collapse which has caused the left mainstem bronchus to assume a more
horizontal course. The atelectasis extends to the hilar region, but does not involve the
entire left lung.
iii) Invades the visceral pleura- T2a
Example 1: This patient presented with a 4.5 cm
carcinosarcoma in the right upper lobe. The lesion abutted the chest wall along its
superior margin (blue arrows). At resection, the tumor invaded the visceral pleura, but
the parietal pleura had no evidence of involvement.
Example 2: This is an interesting example of visceral
pleural invasion. In this case of adenocarcinoma there are thin stands of density which
are seen radiating from the lesion to the pleural surface where there is a focal
plaque-like soft tissue mass (yellow arrows). On histopathologic analysis there was
visceral pleural extension of the primary lesion (making the lesion T2a), but the pleural
soft tissue mass proved to be fibrous tissue and scar. Thus, the primary lesion does not
necessarily need to be in direct contact with the pleura to have invasion.
NOTE: To load a higher resolution
view, simply click directly on the image below.
T3: A tumor over 7 cm in size; or of any size that directly invades any
of the following: the chest wall (including superior sulcus tumors and those
with rib destruction), diaphragm, mediastinal pleura, parietal pericardium, or phrenic nerve; tumor in the main bronchus less than 2 cm distal
to the carina (but without involvement of the carina); tumor associated with atelectasis
or obstructive pneumonitis of the entire lung; or a tumor with a satellite
tumor nodule in the same primary tumor lobe. Previously, a
satellite tumor nodule in the same primary lobe was classified as T4, but
the 5-year survival in these patients is 28%- which is similar to the 31%
survival for other T3 lesions.
Example 1: T3 lesion- chest wall invasion. This patient
presented with a long history of shoulder and neck pain. An abnormality was detected on
CXR and a CT scan confirmed the presence of a superior sulcus tumor (an adenocarcinoma)
associated with chest wall invasion and rib destruction (yellow arrows). Rib involvement
does not preclude surgical resection in patients with superior sulcus tumors.
Example 2: The T3 lesion below was a squamous cell
carcinoma in the right main bronchus that was within 2 cm of the carina. There is some
associated right upper lobe atelectasis.
Example3: T3 lesion with entire lung collapse. This
patient with non-small cell lung cancer demonstrates an abrupt cut off of the left
mainstem bronchus (black arrows) with complete left lung collapse due to a large
endobronchial mass.
Example 4: This patient with adenocarcinoma
of the superior segment of the left lower lobe (yellow arrow) was also noted to have a
stellite nodule in the ipsilateral tumor lobe (white arrow) adjacent to the major fissure.
This is now a T3 lesion by the new staging system.
T4: A tumor of any size that invades any of the
following: mediastinum, heart, great vessels, trachea, esophagus, vertebral body, carina,
or recurrent laryngeal nerve. Also- tumor nodules in another
ipsilateral lobe (not in the primary tumor lobe) are now considered T4
(previously classified as M1).
Example 1: This patient with bronchogenic carcinoma had a
large central mass that was directly invading the superior vena cava (yellow arrows).
Lesions that invade the great vessels are considered T4:
NOTE: To load a higher resolution view, simply click
directly on the image below.
Example 2: This is an example of a T4
lesion in a patient with NSCLC that was invading a thoracic vertebral body. The rib is
also involved.
Example 3: This patient with adenocarcinoma had a large
mass which was obstructing the left upper lobe bronchus causing left upper lobe collapse.
The large left pleural effusion was positive for malignant cells making this a T4 lesion.
Other important findings which indicate non-resectability in this case include encasement
of the left pulmonary artery to it's origin from the main pulmonary artery.
NOTE:
To load a higher resolution view, simply click directly on either image below.
Example 4: This patient with non-small cell lung cancer
had a necrotic tumor (M) which was involving the carina (T4 lesion). A virtual bronchoscopic image is also provided -- the mass is indicated by the blue arrows.
NOTE: To load a higher resolution
view, simply click directly on either image below.
Example 6: This patient had a superior sulcus tumor
(yellow arrows) that was invading into the mediastinum. Note the loss of a fat plane
between the mass and the esophagus (white arrows). Esophageal encasement is demonstrated
on the barium swallow (black arrows). This is another example of a T4 lesion.
NOTE: To load a higher
resolution view, simply click directly on the image below.