International Staging System for Lung Cancer
The International Staging System for Lung
Cancer provides a common framework for the discussion of patients with bronchogenic
carcinoma. More importantly, however, patient treatment options and prognosis are directly
related to their tumor stage at presentation. The staging system is derived from a TNM
classification scheme (T=primary tumor, N= regional lymph nodes, M= distant metastasis)
with four separate stage groups from I to IV. Stage I reflects the best prognosis, stage
IV the worst. Prior to discussion of specific stages, one must understand the TNM
descriptors.
TNM Descriptions
(From: Chest 1997; Mountain CF. Revisions in
the international system for staging lung cancer. 111: 1710-17)
Primary Tumor (T)
"T" describes the primary tumor in terms of size
and involvement. There are four "T" classifications that are commonly applied
(T1 through T4):
T1: A tumor less than or equal to 3 cm in greatest
dimension, surrounded by lung or visceral pleura, without bronchoscopic evidence of
invasion more proximal than the lobar bronchus (i.e., not in the main bronchus)
T2: A tumor with any of the following
features:
- Larger than 3 cm in largest dimension
- Involvement of the mainstem bronchus, but is greater
than 2 cm from the carina
- Invades the visceral pleura
- Associated with atelectasis or post-obstructive pneumonitis
that extends to the hilar region, but does not involve the entire lung
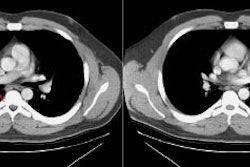
T3: A tumor of any size that directly invades any
of the following: the chest wall (including superior sulcus tumors), diaphragm,
mediastinal pleura, parietal pericardium; tumor in the main bronchus less than 2 cm distal
to the carina (but without involvement of the carina); tumor associated with atelectasis
or obstructive pneumonitis of the entire lung.
T4: A tumor of any size that invades any of the
following: mediastinum, heart, great vessels, trachea, esophagus, vertebral body, carina;
any tumor with a malignant pleural or pericardial effusion; or any tumor with satellite
tumor nodules within the ipsilateral primary-tumor lobe of the lung.
Other primary tumor descriptors which are less commonly
applied include:
- TX: A primary tumor cannot be assessed, or tumor proven by
the presence of malignant cells in sputum or bronchial washings, but not visualized by
imaging or bronchoscopy.
- T0: No evidence of a primary tumor
- TIS: Carcinoma in situ
Regional Lymph Node Status (N)
There are four "N" classifications that are
commonly applied (N0 through N3):
N0: No regional lymph node metastasis
N1: Ipsilateral peribronchial or hilar nodal
metastases; or intrapulmonary nodes involved by direct extension of the primary tumor. All
N1 nodes lie distal to the mediastinal pleural reflection.
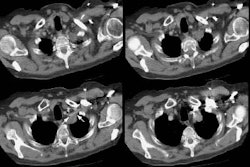
N2: Ipsilateral mediastinal and subcarinal lymph
nodal metastases. Midline pre-vasuclar and retrotracheal nodes are considered ipsilateral
[5], while nodes to the contralateral side of midline are considered N3 (verbal
communication Clifton F. Mountain, MD, Division of Cardiothoracic Surgery, The University
of California Medical Center at San Diego). Although subcarinal nodes may extend into the
contralateral mediastinum, they are generally considered to be N2.
N3: Contralateral mediastinal or contralateral
hilar nodal metastases; also includes ipsilateral or contralateral scalene or
supraclavicular nodes. Supraclavicular lymph node metastases are found more
frequently in patients with N2 or N3 disease [155]. Up to 53% of patients
with enlarged N3 nodes will have supraclavicular nodal metastases [155]. Other cervical nodes are classified M1 [5].
NX: Regional lymph nodes cannot be assessed
Distant Metastasis (M)
M0: No distant metastasis
M1: Distant metastasis present; or separate tumor
nodules in the ipsilateral nonprimary-tumor lobes of the lung. Separate tumor nodules in
the contralateral lung are considered M1 if they are of the same histologic cell type as
the primary lesion. A contralateral lung tumor with a different cell type is considered a
synchronous primary lesion and should be staged independently (Verbal communication Dr.
Clifton F. Mountain, MD, Division of Cardiothoracic Surgery, The University of California
Medical Center at San Diego).
MX: Presence of distant metastasis
cannot be assessed
Staging of
Bronchogenic Carcinoma
Clinical staging (pre-operatively) is denoted
by the prefix "c" prior to the TNM designation, while a "p" indicates
the surgical-pathologic staging.
The new classification system shown below
reflects the following modifications from the previous staging system:
Whereas T1N0M0 and T2N0M0 tumors were previously
classified as Stage I, they are now considered separately as Stage IA (T1N0M0), and Stage
IB (T2N0M0) lesions, respectively. Similarly, Stage II has also been sub-divided into a
Stage IIA (T1N1M0) and IIB (T2N1M0). T3N0M0 lesions were previously considered Stage IIIA,
but they are now classified as Stage IIB. These changes were made in order to more
accurately reflect prognostic implications.
New rules were also established for
classifying multiple tumor nodules. The presence of satellite tumor nodule(s) within the
ipsilateral primary tumor lobe are classified as T4, while intrapulmonary ipsilateral
metastases in a non-primary tumor lobe are considered M1.
| Stage |
Tumor |
Nodes |
Metastases |
Stage 0
|
TIS- Carcinoma in situ |
|
|
| IA IB
|
T1 T2
|
N0 N0
|
M0 M0
|
| IIA IIB
|
T1 T2
T3
|
N1 N1
N0
|
M0 M0
M0
|
| IIIA |
T1 or T2 T3
|
N2 N1 or N2
|
M0 M0
|
| IIIB |
Any T T4
|
N3 Any N
|
M0 M0
|
IV
|
Any T |
Any N |
M1 |
|