Lipoma:
Clinical:
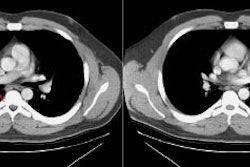
Pulmonary lipomas are most commonly endobronchial (80%), but endobronchial lipomas (or lipomatous hamartomas) are very rare tumors (accounting for only 0.1% of all pulmonary tumors and about 3 to 9% of all benign endobronchial tumors [3]). The majority of lesions are pedunculated and arise from the submucosa of the main or segmental bronchi. Tracheal lesions are rare [4]. Most affected patients are late middle age and there is a male predominance [4]. Lipomas can produce symptoms of airway obstruction with cough, wheezing, recurrent pneumonia, and brochiectasis [6]. The lesion is minimally vascular, but hemoptysis can be a presenting symptom [4]. Treatment of choice is bronchoscopic or surgical resection.X-ray:
The lesion itself is generally not visible on plain film, but the indirect signs of endobronchial obstruction such as atelectasis, infection, or air-trapping are more apparent. CT can be used to demonstrate the fatty nature of the lesion.REFERENCES:
(1) J Comput Assist Tomogr 1991; Mata JM, et al. Endobronchial lipoma: CT diagnosis. 15 (5): 750-751
(2) AJR 1999; Raymond GS. Endobronchial lipoma: Helical CT diagnosis. 173: 1716 (No abstract available)
(3) Radiographics 2002; Gaerte SC, et al. Fat-containing lesions of the chest. 22: S61-S78
(4) AJR 2006; Ko JM, et al. Benign tumors of the tracheobronchial tree: CT-pathologic correlation. 186: 1304-113
(5) Radiographics 2008; Martinez S, et al. Mucoid impactions: finger-in-glove sign and other CT and radiographics features. 28: 1369-1382
(6) Radiographics 2009; Park CM, et al. Tumors in the tracheobronchial tree: CT and FDG PET features. 29: 55-71