Patient positioning plays a key role in the effectiveness of directed prostate biopsy with high-frequency Doppler ultrasound, according to researchers from Thomas Jefferson University in Philadelphia.
In the latest issue of Radiology, Dr. Ethan Halpern and colleagues from the Jefferson Prostate Diagnostic Center set out to investigate several issues. They sought to evaluate cancer detection with directed biopsy of the prostate on the basis of high-frequency Doppler ultrasound findings, compare the findings with those of standard sextant biopsy, and finally, determine if the position of the patient during the ultrasound-guided biopsy had any effect on the observed flow pattern.
"Approximately 15%-35% of cancers are missed with conventional sextant biopsy. Color Doppler ultrasonography with directed biopsy may increase the number of cancers detected," the authors wrote (Radiology, March 2002, Vol.222:3, pp. 634-639).
With regard to patient positioning, "early in the course of this study, it became apparent that focally increased flow was present in many patients (predominantly on the left side of the prostate) and was not associated with the presence of malignancy," they said.
Thirty-two consecutive patients with prostate specific antigen (PSA) levels ranging from 2.3 to 28 ng/mL were enrolled in the study. Grayscale, color Doppler, and power Doppler transrectal ultrasonography were performed with each patient in the left lateral decubitus position. All exams were done with an EC10C5 end-fire probe and the Sequoia 512 super-premium general imaging scanner (Acuson, Mountain View, CA). The probe center frequency was 10 MHz for the grayscale ultrasound and 9 MHz for the color and power Doppler ultrasound.
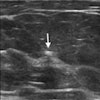
The color and power Doppler images were evaluated for the presence of increased flow within the parenchyma of the prostate, and were graded on a 5-point scale ranging from definitely abnormal (5) to normal (1). Biopsy was performed directly after grayscale and Doppler ultrasound. An 18-gauge core biopsy needle was used to obtain four specimens from each patient.
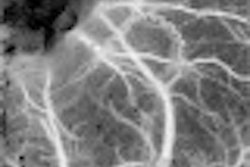
According to the results, "significantly more flow was visualized at the base of the gland than at the apex with both color and Doppler ultrasound." As a result, of the 90 directed biopsy cores obtained in the patient population, 62 were obtained in the left base and midgland because of increased Doppler flow in these areas. On the basis of color Doppler findings, 50 out of the 62 samples were rated indeterminate (score of 3) or abnormal (4 or 5). Based on power Doppler imaging, 57 cores were given a 3-5 rating. On grayscale, 25 out of 62 were rated between 3 and 5.
"In all, 24 positive biopsy cores were obtained in seven patients. Sextant biopsy results were positive in 16 of 192 cores (8%). Directed biopsy results were positive in 8 of 90 cores (9%). All seven cases of cancer were identified with sextant biopsy, but only four were identified with directed biopsy," the article stated.
The authors concluded that the positive biopsy yield of both approaches were similar, especially as the ultrasound-directed biopsy did not show any additional cancers in this patient population. In order to evaluate a relationship between these findings and patient positioning, three of the study’s authors volunteered to have their healthy prostates imaged. Each subject was scanned in the left lateral decubitus, right lateral decubitus, and supine positions.
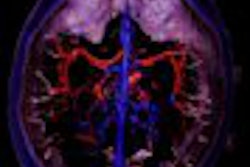
"In the left lateral decubitus position, increased Doppler flow was demonstrated in the left base and midgland compared with that in the right side. The flow distribution shifted toward the right side when each subject was evaluated in the right lateral decubitus position. A more symmetric flow pattern was demonstrated with each subject in the supine position," the investigators reported.
Halpern and co-authors suggested that Doppler ultrasound should not be performed with the patient in a decubitus position, but rather in a supine position for a more symmetric flow pattern.
As the flow increased to the dependent side of the prostate, regardless of whether the patient was healthy or not, physicians who performed biopsies should be aware of this effect of patient position on ultrasound-guided biopsy, they concluded.
By Shalmali PalAuntMinnie.com staff writer
March 20, 2002
Related Reading
Lidocaine decreases pain of ultrasound-guided needle biopsy of the prostate, February 11, 2002
BioPince needle has pros and cons for prostate biopsy, February 2, 2002
Ultrasound has prostate cancer in its crosshairs, March 14, 2001
Copyright © 2002 AuntMinnie.com