Lymphoma in HIV:
Clinical:
Patients with HIV infection are at an increased risk for lymphoma
(AIDS related lymphoma)- nearly a 12 to 200 fold increased risk
over the general population [7,8,9]. Lymphoma in the HIV
population develops at a younger age (37 years vs 65 years for the
general population) [9]. The risk for lymphoma is highest in
patients with moderate immunosuppression and the risk decreases
with decreasing CD4 count below 200 cells/uL [7]. Since the
introduction of HAART, non-Hodgkins lymphoma has become less
common- estimates are that 5-20% of HIV patients undergoing HAART
therapy will eventually have lymphoma [9].
Lymphoma develops in 3 to 20% of HIV patients and 90% of the
lesions are non-Hodgkins lymphomas (typically highly aggressive
multi-clonal B-cell) [2,6,9]. An association with Ebstein-Barr
virus or the c-myc gene has been postulated. The Ebstein-Barr
virus genome is identified in 50-85% of AIDS related non-Hodgkin's
lymphomas [2,5]. Nearly three-quarters of patients present with
advanced stage disease (Stage III or IV). Lymphoma in HIV patients
is very often extranodal 984-90% of patients [4,9], most commonly
involving the central nervous system, gastrointestinal tract, or
bone marrow [9]. Primary intrathoracic disease is uncommon (less
than 10% of patients). HIV-Lymphoma occurs in more advanced stages
of immune suppression- when the CD4 level is under 100 cells/uL
[2]. Most patients have systemic symptoms of fever, night sweats,
or weight loss. The majority of patients with systemic AIDS
related NHL have one of three high grade B-cell lymphomas- Burkitt
lymphoma, diffuse large B-cell lymphoma with centroblastic
features, and diffuse large B-cell lymphoma with immunoblastic
features [5].The prognosis in these patients is poor with an
average survival of 5 months after diagnosis.
Burkitt lymphoma occurs in HIV-patients with a high CD4 count
(> 200 cells/uL) [8].
Hodgkins lymphoma occurs up to 8 times more frequently in HIV patients and it is also strongly linked to Epstein-Barr virus infection [4,5]. It is usually of an aggressive histologic subtype - the mixed cellularity and lymphocyte depleted subtypes are most common [4,5]. At the time of diagnosis, the majority of patients present with B-symptoms [8]. It also has a higher incidence of extranodal involvement including the bone marrow (40-50%), liver (15-40%), and spleen (20%) [5,8]. HIV patients with Hodgkins lymphoma have a much worse prognosis than the general population [4]. Hodgkins lymphoma tends to occur early in AIDS, usually when the CD4 count is greater than 200 cells/uL (275-306 cells/uL) [2,8].
Body cavity-based lymphoma is a rare form of AIDS related B-cell lymphoma.
X-ray:
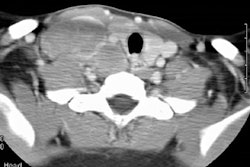
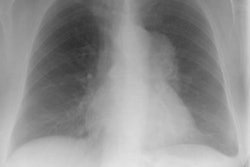
Radiography: Disease in the thorax is typically extranodal, with parenchymal disease and pleural effusions (in 25-73%) found more commonly than adenopathy (hilar/mediastinal adenopathy is seen in only 20-30% of these cases). Diffuse, often peripheral, well-defined nodules are the most common pulmonary parenchymal presentation, although lymphoma in HIV can present as a solitary well defined nodule [2]. Masses may cavitate in up to 10% of cases. Dense airspace consolidation may also be identified. Endobronchial lesions may also occur [5].
Scintigraphy: Pulmonary lymphoma in HIV patients typically accumulated both gallium and thallium.
REFERENCES:
(1) AJR 1997; Au V, Leung AN. Radiologic manifestations of lymphoma in the thorax. 168: 93-98 (No abstract available)
(2) Radiologic Clinics of North America 1997; McGuinness G. Changing trends in the pulmonary manifestations of AIDS. 35 (5): 1029-1082
(3) Radiology 1998; Collins J, et al. Epstein-Barr-virus-associated lymphoproliferative disease of the lung: CT and histologic findings. 208: 749-759
(4) AJR 2007; Burns J, et al. Oncogenic viruses in AIDS:
mechanisms of disease and intrathoracic manifestations. 189:
1082-1087
(5) AJR 2011; Davison JM, et al. FDG PET/CT in patients with HIV.
197: 284-294
(6) AJR 2012; Lichtenberger JP, et al. What a differetial a virus
makes: a practical approach to thoracic imaging findings in the
context of HIV infection- Part 2, extrapulmonary pulmonary
findings, chronic lung disease, and immune reconstitution
syndrome. 198: 1305-1312
(7) Radiographics 2014; Chou SHS, et al. Thoracic diseases
associated with HIV infection in the era of anti-retroviral
therapy: clinical and imaging findings. 34: 895-911
(8) Radiographics 2018; Javadi S, et al. HIV-related malignancies
and mimics: imaging findings and management. 38: 2051-2068
(9) AJR 2021; Glushko T, et al. HIV lymphadenopathy: differential diagnosis and important imaging features. 216: 526-533