VIENNA - While medical textbooks and scientific papers tend to favor the use of MRI for staging head and neck cancer, CT provides more relevant diagnostic information in most cases, according to Dr. Dirk Pickmuth from Martin Luther University in Halle-Wittenberg, Germany. In a study presented yesterday at the European Congress of Radiology, Pickmuth said CT provides the most accurate staging information in a single exam.
"The morbidity and mortality of head and neck tumors is very high, as we know, and it's quite important to stage it accurately with either CT, MRI, or both," Pickmuth said. "The T and N staging of the tumor is very important to guide the treatment of these patients, and that influences the survival rate. It is especially important to determine the tumor margins with respect to anatomic landmark structures."
So in an effort to evaluate the accuracy of CT and MRI staging of head and neck tumors -- and determine which modality provides the most relevant staging information in a single exam -- the team worked with otorhinolaryngologists at their institution to develop a new standardized information protocol and a clinically oriented reporting protocol, Pickmuth said.
To determine the N stage of tumors, they used an imaging-based classification system employed by the American Academy of Otolaryngology, Head and Neck Surgery. The protocols emphasize the specific information that radiologists must convey to clinicians, according to Pickmuth.
"The tumor origins included the oropharynx, oral cavity, floor of the mouth, hypopharynx, and pharynx tumors, and 82% of them were squamous cell carcinomas," he said.
In the study, 50 consecutive patients with head and neck cancer underwent both CT and MRI within 1-2 days of each other.
CT was performed with either single-slice or multislice spiral CT, with axial and coronal sections of soft tissue and bone in all patients. MRI was conducted with both 1- and 1.5-tesla scanners, with a spin-echo protocol and fat-suppression techniques in the axial, coronal, and sagittal planes, both pre- and post-contrast.
"The resulting images were independently reviewed by three radiologists, and the findings were correlated with operative and histopathologic findings," he said.
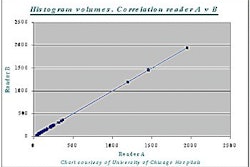
The radiologists assessed tumor volume, local extent, spread into soft tissues, invasion into bony structures, relationship to neurovascular bundles (of special concern to surgeons), extension across midline, and lymph node involvement.
The main problem with the CT scans were dental fillings, which resolved nicely in the MRI studies, Pickmuth said. The main problem with MRI was motion artifacts, due to patient movement, respiration, coughing, and swallowing. In all, motion artifacts degraded 6% of MRI studies.
The overall accuracy of CT was 86%, compared with 82% for MRI. Sensitivity was 93% for CT, and 95% with MRI. Specificity was significantly higher in CT (85%) than in MRI (66%).
"N staging was rather poor with both techniques: 83% with CT, 72% with MRI," Pickmuth said. "There was a high rate of understaging with both modalities, ranging from 23% to 25%.... The clinicians found a lot of pathological lymph nodes, more than we did in our radiological CT and MRI reports."
CT was less sensitive but more specific than MRI in the detection of head and neck tumors, Pickmuth said. As shown in previous studies, CT was superior in the assessment of bone invasion, while MRI had better soft-tissue contrast.
"We think that in this era of cost concerns, it's a good principle to do just one examination, and because of the cost and availability of the machines, we think that CT should be the method of choice," he said. MRI should be added if necessary to resolve unanswered questions regarding issues such as submucosal spread and muscle invasion.
An audience member said that comparisons of CT and MRI and outcomes of the comparisons would certainly vary greatly depending on tumor type.
"That's the major drawback of the study," Pickmuth said. However, there weren't enough patients to segregate subgroups by tumor type. He said it took a full year to get 50 consecutive patients who underwent both exams, and that the study is ongoing.
"I'm absolutely convinced that there will be subgroups where one method will be better than the other," he said.
By Eric Barnes
AuntMinnie.com staff writer
March 3, 2001
Click here to post your comments about this story. Please include the headline of the article in your message.
Copyright © 2001 AuntMinnie.com