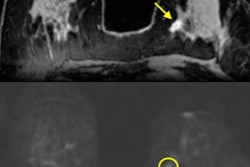
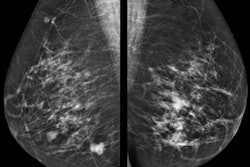
VIENNA - Mammography and ultrasound underestimate 30% of disease in patients with invasive ductal carcinoma (IDC), according to research from Israel presented at ECR 2018. MRI overestimates the extent of disease, but at least no cancer is left behind.
IDC constitutes 70% to 85% of breast cancers, according to Dr. Tamar Sella from Hadassah Medical Center in Jerusalem. Invasive lobular carcinoma (ILC) is the second most common subtype, occurring in 5% to 15% of patients. ILC is also more frequently multifocal, multicentric, and bilateral with a high discordant rate between imaging and pathology.
"There is obviously a need for more accurate imaging presurgically," Sella told a packed audience at ECR.
Numerous studies have shown that MRI benefits ILC evaluation both for lesion detection and evaluation of the extent of disease, but limited literature exists that compares the modality with mammography and ultrasound, she said.
"There is even more restricted literature comparing these various modalities specifically to the two larger subgroups of disease -- IDC, ILC," she added.
Therefore, she and her colleagues evaluated the incremental value of preoperative breast MRI over mammography and ultrasound in depicting the accurate extent of disease specifically in IDC and ILC regarding multifocality and multicentricity of disease.
The researchers retrospectively examined 239 patients with newly diagnosed breast cancer. Almost all patients had mammography available for review, and almost all had ultrasound performed at the institution and available for review. All patients had routine clinical 3-tesla MRI, and surgical pathology was the reference standard.
IDC constituted about 80% of the study group and ILC 20%, so the proportions mirrored the general population. The overall concordance rate for all three imaging modalities was relatively similar, between 65% and 75%, the researchers found. Most concordance cases had only unifocal disease, with a minority showing multifocal disease. Mammography and ultrasound tended to underestimate focality of disease, whereas MRI overestimated disease. The same was true regarding multicentricity in IDC, with an equal proportion of 76% concordance between all three imaging modalities. However, in the 25% discordance, mammography and ultrasound underestimated disease whereas MRI overestimated disease more commonly.
ILC told a different story: MRI demonstrated a much higher concordance compared with mammography and ultrasound. In mammography and ultrasound, the concordance rate was less than 50%.
"We were missing additional foci in over 50%," Sella said. "Regarding those cases with discordance, in MRI, of course, it was almost 90% concordance. Regarding cases with discordance, again mammography and ultrasound underestimated disease and discordance was very rare for MRI, so it doesn't really matter if it over- or underestimates."
In terms of multicentricity in ILC, the trend continued: Mammography and ultrasound underestimated disease extent and MRI overestimated it.
"The added benefit of MRI for evaluation of the extent of disease is clearly greater in ILC than IDC, demonstrating an 80% to 90% concordance rate with pathology," she said. "We suggest that MRI should routinely be included in preoperative evaluation of patients with ILC."
During the question and answer period, Sella said that even though there was an equal concordance rate between the different modalities for IDC, she would still recommend MRI in order not to underestimate disease in the vast majority of patients with breast cancer.