F-18 fluoroestradiol (FES) PET/CT has excellent specificity and moderate sensitivity for diagnosing axillary lymph node metastasis in women with invasive lobular cancer, a group in South Korea has reported.
The finding is from a prospective phase II feasibility study involving 20 women and suggests the technique holds promise for improving surgical plans in newly diagnosed patients, noted lead author Jeongryul Ryu, PhD, of the University of Ulsan in Seoul, and colleagues.
“This study serves as the first feasibility analysis investigating the potential utility of F-18 FES PET/CT as a staging modality in early-stage [invasive lobular cancer],” the group wrote. The work was published August 14 in the Journal of Nuclear Medicine.
Invasive lobular breast cancer (ILC) is the second most prevalent type of breast cancer, representing approximately 15% of all invasive breast cancers. ILC grows in a linear pattern through the breast without distorting the surrounding structures or forming a lump and thus is difficult to detect on mammography, ultrasound, MRI, and F-18 FDG-PET, the authors explained.
Conversely, F-18 FES radiotracer (Cerianna, GE HealthCare) binds to estrogen receptors on ILC cells and was approved in the U.S. in 2020 for diagnosing distant metastasis or recurrence in patients with estrogen receptor-positive breast cancers, such as ILC, they added. Yet to date, there is a lack of evidence from prospective clinical trials for initial staging, the researchers noted.
To that end, the group conducted a phase II single-center prospective feasibility trial. They enrolled 20 women (median age, 52) with newly diagnosed estrogen receptor-positive ILC. Subjects had a confirmed or suspected axillary lymph node (ALN) metastasis on physical examination or imaging and were scheduled to undergo axillary surgery.
All patients underwent F-18 FES PET/CT (Biograph Vision, Siemens Healthineers) within 90 days of their initial diagnosis via biopsy, with the scans interpreted visually and semiquantitatively within a few days of acquisition compared with surgical specimens.
According to the results, out of the 20 subjects, 12 had proven ALN metastasis. On visual analysis, F-18 FES PET/CT showed a sensitivity of 67% (8/12) and a specificity of 100% (8/8). There were four false-negative cases, all of whom had a single metastasis on the sentinel lymph node, and the researchers detected an unexpected F-18 FES-positive ipsilateral internal mammary lymph node in one patient.
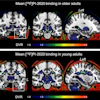
 A 58-year-old woman was diagnosed with ER-positive (Allred score 8) ILC in her right breast. Ultrasound and MRI found prominent lymph nodes in right axillary level I area, diagnosed as metastasis on ultrasound-guided fine-needle aspiration. F-18 FES-PET/CT showed a positive mass in right breast (white arrow; SUVmax, 5.6) and multiple F-18 FES–positive lymph nodes in right axillary level I, II, and II/III junction areas (red arrows; SUVmax, up to 12.2). In addition, a small F-18 FES-positive lymph node was observed in the right second internal mammary area (red circles; SUVmax, 1.8). However, biopsy could not be performed because it was too small and not visible on ultrasound; the clinician decided to include internal mammary lymph node in treatment field for adjuvant radiotherapy. The patient underwent lumpectomy with ALN dissection, with five metastases being identified in 13 lymph nodes dissected, and is scheduled to receive adjuvant chemotherapy, radiotherapy, and endocrine therapy.Journal of Nuclear Medicine
A 58-year-old woman was diagnosed with ER-positive (Allred score 8) ILC in her right breast. Ultrasound and MRI found prominent lymph nodes in right axillary level I area, diagnosed as metastasis on ultrasound-guided fine-needle aspiration. F-18 FES-PET/CT showed a positive mass in right breast (white arrow; SUVmax, 5.6) and multiple F-18 FES–positive lymph nodes in right axillary level I, II, and II/III junction areas (red arrows; SUVmax, up to 12.2). In addition, a small F-18 FES-positive lymph node was observed in the right second internal mammary area (red circles; SUVmax, 1.8). However, biopsy could not be performed because it was too small and not visible on ultrasound; the clinician decided to include internal mammary lymph node in treatment field for adjuvant radiotherapy. The patient underwent lumpectomy with ALN dissection, with five metastases being identified in 13 lymph nodes dissected, and is scheduled to receive adjuvant chemotherapy, radiotherapy, and endocrine therapy.Journal of Nuclear Medicine
“In this prospective feasibility study, F-18 FES PET/CT exhibited favorable diagnostic performance for ALN metastasis in patients with ILC, with moderate sensitivity and excellent specificity and [positive predictive value],” the group wrote.
Currently, ultrasound-guided fine-needle aspiration or core-needle biopsy serves as the initial step for axillary staging in patients with ILC breast presenting with clinically suspicious lymph nodes, yet preoperative identification is achieved in only about 50% of women with axillary involvement, the group noted.
Thus, F-18 FES PET/CT presents a promising alternative to meet an unmet clinical need for accurate detection, they suggested.
“F-18 FES PET/CT had excellent specificity and moderate sensitivity for the detection of ALN metastasis in ILC, suggesting its potential as a valuable preoperative staging modality in patients with ILC with clinically suspicious ALNs,” the researchers concluded.
The full study can be found here.