Both standard and ultrahigh resolution modes are effective for coronary CT angiography (CCTA) performed by photon-counting detector CT (PCCT) -- but ultrahigh has an extra advantage in patients with severe coronary artery disease, researchers have found.
The findings will help clinicians optimize protocols for PCCT CCTA, according to a team led by Mengzhen Wang, MD, of Shanghai Jiao Tong University School of Medicine in China.
"For coronary CTA performed by photon-counting detector (PCD) CT, diagnostic performance for significant stenosis is optimized through acquisition in ultrahigh resolution (UHR) mode with reconstruction at 0.2-mm slice thickness," the American Journal of Roentgenology noted in a statement about the study, which was published July 3.
CCTA is a widely used tool for evaluating the presence and severity of coronary artery disease, but its diagnostic efficacy is lower in patients with extensive coronary artery calcification, the team explained. That's where PCCT comes in: The technology offers higher contrast-to-noise ratio and spatial resolution than conventional CT imaging.
In their study, Wang and colleagues assessed the diagnostic performance for detecting stenosis on CCTA performed by PCCT with various standard resolution and ultrahigh resolution protocols. The group used invasive coronary angiography (ICA) as the reference standard.
The research included a total of 122 inpatients who underwent CCTA between October 2023 and October 2024; of these, 61 patients underwent exams with a standard resolution protocol and 61 with an ultrahigh resolution protocol. The patients also underwent ICA.
The exams were reconstructed in the following manner:
- Standard resolution: "SRnormal" and "SRVNCa" (virtual noncalcium) image sets, both using 0.6-mm slice thickness and Bv40 kernel.
- Ultrahigh resolution: "UHRnormal" (0.6-mm slice thickness, Bv40) and "UHRthin" (0.2-mm slice thickness, Bv64) image sets.
Two radiologists measured the diameters of any stenoses; these were considered significant at a threshold equal to or greater than 50%.
Per-segment CCTA interpretation performance by reader | ||
Measure | Reader 1 | Reader 2 |
SRnormal | ||
| Sensitivity | 92.9% | 92.9% |
| Specificity | 89.9% | 88.8% |
| Accuracy | 90.5% | 89.6% |
SRVNCa (virtual calcium) | ||
| Sensitivity | 92.9% | 93.5% |
| Specificity | 91.6% | 92.3% |
| Accuracy | 91.9% | 92.5% |
UHRnormal | ||
| Sensitivity | 96% | 96% |
| Specificity | 92.4% | 91.6% |
| Accuracy | 93% | 92.2% |
UHRthin | ||
| Sensitivity | 100% | 100% |
| Specificity | 98.6% | 98.9% |
| Accuracy | 98.8% | 99% |
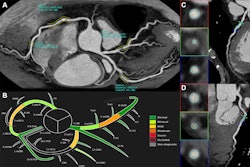
 72-year-old female participant with heart failure. Patient underwent coronary CTA by photon-counting detector CTA, acquired in UHR mode. Agatston score was 1,615. Heart rate was 59 beats/min. (A) Reconstructed UHRnormal image. Proximal RCA shows calcified plaque. Inset shows cross-section of RCA at level of thin line traversing vessel. (B) Reconstructed UHRthin image. Proximal LCX shows calcified plaque. Inset shows cross-section of RCA at level of thin line traversing vessel. Insets show less blooming artifact from calcified plaque for UHRthin than for UHRnormal. Stenosis at site of calcification was measured as 60% for UHRnormal and 30% for UHRthin. (C) Image from subsequent invasive coronary angiography shows 30% stenosis of RCA (arrow). UHR = ultrahigh resolution. Images and caption courtesy of the AJR.
72-year-old female participant with heart failure. Patient underwent coronary CTA by photon-counting detector CTA, acquired in UHR mode. Agatston score was 1,615. Heart rate was 59 beats/min. (A) Reconstructed UHRnormal image. Proximal RCA shows calcified plaque. Inset shows cross-section of RCA at level of thin line traversing vessel. (B) Reconstructed UHRthin image. Proximal LCX shows calcified plaque. Inset shows cross-section of RCA at level of thin line traversing vessel. Insets show less blooming artifact from calcified plaque for UHRthin than for UHRnormal. Stenosis at site of calcification was measured as 60% for UHRnormal and 30% for UHRthin. (C) Image from subsequent invasive coronary angiography shows 30% stenosis of RCA (arrow). UHR = ultrahigh resolution. Images and caption courtesy of the AJR.
The key finding of the work was that both standard resolution and ultrahigh resolution PCCT achieved high diagnostic performance for significant stenosis using ICA as the reference standard -- although the team did note that "the superior diagnostic performance of UHR mode was most evident in patients with heavily calcified vessels," writing that "radiology practices could consider prioritization of UHR mode for patients with known extensive coronary calcification or with strong clinical suspicion for severe CAD."
The complete study can be found here.