Coronary artery calcium (CAC) scoring with CT could determine whether patients with heart disease symptoms are at low risk of heart attacks or strokes, according to a study published March 5 in Radiology.
The study results could help patients with stable chest pain avoid invasive coronary angiography (ICA), said senior author Marc Dewey, MD, of Charité - Universitätsmedizin Berlin in Germany in a statement released by the RSNA.
"[Our] findings suggest that patients with stable chest pain and a coronary artery calcium score of zero may not require invasive coronary angiography using cardiac catheterization because the risk of cardiovascular events is so low," Dewey said.
CAC scoring with CT is a noninvasive method for measuring the amount of calcium in the heart arteries, noted a team led by doctoral candidate Federico Biavati, MD, also of Charité. Scores between one and 399 suggest a moderate amount of plaque and those of 400 or higher suggest a large plaque burden. Conversely, the absence of CAC tends to be a reliable indicator of the absence of advanced atherosclerosis.
But the role of CAC in patients with stable chest pain remains unclear, Biavati and colleagues explained. To address this knowledge gap, the group conducted a study that explored the prognostic value of CAC scoring for major adverse cardiovascular events in 1,749 individuals with low CAC scores, using data from the Diagnostic Imaging Strategies for Patients With Stable Chest Pain and Intermediate Risk of Coronary Artery Disease (DISCHARGE) trial.
Study participants had stable chest pain and were referred for ICA. They were grouped into low-, intermediate- and high-risk categories based on their CAC scores and tracked for an average of 3.5 years for any major adverse cardiovascular events.
The researchers found the following:
- The 755 participants with a CAC score of 0 showed a 0.5% risk rate of major adverse cardiovascular events.
- In the 743 participants with CAC scores of 1 to 399, there were 14 major adverse cardiovascular events, for a risk rate of 1.9%.
- In the 251 participants with CAC scores of 400 or higher, there were 17 major adverse cardiovascular events, for a risk rate of 6.8%.
The team also reported that the prevalence of obstructive coronary artery disease (CAD) at CT angiography rose from 4.1% in the CAC score 0 group to 76.1% in the CAC score 400 or higher group.
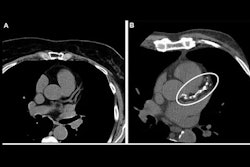
 Example axial noncontrast CT scans in (A, C, E) a participant with a coronary artery calcium (CAC) score of 0, no signs of coronary artery disease at CT, and no major adverse cardiovascular events and (B, D, F) a participant who had a CAC score of 1013 (group with a CAC score of 400 or higher) and obstructive coronary artery disease at CT and required a revascularization procedure. With the scan on the left as reference, calcified plaques (ovals) can be seen on the right scan of the left main and left anterior descending arteries (proximal and midsegment, B) and the right coronary artery (proximal vessel segment, D; middle vessel segment, F). Image courtesy of Radiology.
Example axial noncontrast CT scans in (A, C, E) a participant with a coronary artery calcium (CAC) score of 0, no signs of coronary artery disease at CT, and no major adverse cardiovascular events and (B, D, F) a participant who had a CAC score of 1013 (group with a CAC score of 400 or higher) and obstructive coronary artery disease at CT and required a revascularization procedure. With the scan on the left as reference, calcified plaques (ovals) can be seen on the right scan of the left main and left anterior descending arteries (proximal and midsegment, B) and the right coronary artery (proximal vessel segment, D; middle vessel segment, F). Image courtesy of Radiology.
The study adds to the clinical literature in that it "specifically focused on CAC scoring in a group referred for ICA, which had not been extensively studied," Biavati and colleagues wrote.
"By addressing this group, the trial fills an important research gap and provides valuable insights for patients initially being considered for ICA with stable chest pain and intermediate pretest probability of CAD," they noted.
The results show promise, but more research is needed, wrote Kate Hanneman, MD, of the University of Toronto in Canada, and colleague Gaurav Gulsin, MD, PhD, of the Leicester Biomedical Research Centre in the U.K., in an accompanying commentary.
"Beyond clinical parameters, further study is needed to identify biomarkers of high-risk plaque features and future major adverse cardiovascular events risk in patients with a CAC score of 0," Hanneman and Gulsin concluded.
The complete study can be found here.