A low-dose protocol of intravenous contrast-enhanced 2-mSv CT is comparable to conventional-dose CT for diagnosing right colonic diverticulitis, according to a new research study.
The results could help clinicians better distinguish right colonic diverticulitis from appendicitis, noted a team led by Dr. Hae Young Kim, PhD, of Seoul National University Bundang Hospital in South Korea.
"By mitigating concern of missed diagnosis of right colonic diverticulitis, our results further support the use of low-dose CT for suspected appendicitis," the group wrote in a paper published on 8 April in the American Journal of Roentgenology.
Kim and colleagues performed a study that included 3,074 patients between the ages of 15 and 44 seen at 20 hospitals. The patients were randomized into two groups, one that underwent contrast-enhanced 2-mSv CT (1,535) and another that underwent conventional CT (1,539) between December 2013 and August 2016. A team of 161 radiologists read the exams, recommending alternative diagnoses in 976 of the low-dose CT exams and in 924 of the conventional CT exams.
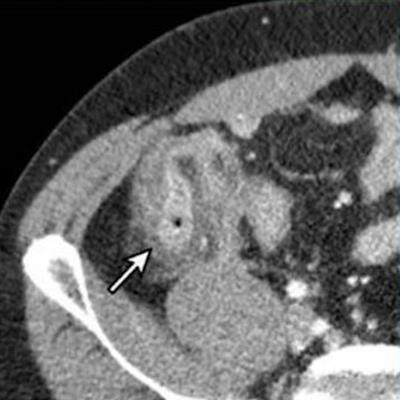
 Intravenous contrast-enhanced 2-mSv 4-mm-thick transverse and coronal (B) CT images show inflamed diverticula (arrows), segmental colonic wall thickening, and adjacent pericolic fat stranding. Images courtesy of the American Roentgen Ray Society and the American Journal of Roentgenology.
Intravenous contrast-enhanced 2-mSv 4-mm-thick transverse and coronal (B) CT images show inflamed diverticula (arrows), segmental colonic wall thickening, and adjacent pericolic fat stranding. Images courtesy of the American Roentgen Ray Society and the American Journal of Roentgenology.The researchers found that true positives, true negatives, sensitivity, and specificity results between the two groups were not statistically significant, demonstrating the efficacy of low-dose CT for this indication, they concluded.



















