The Society of Cardiovascular Computed Tomography (SCCT) published a new consensus document on coronary CT angiography (CTA) in the Journal of Cardiovascular Computed Tomography.
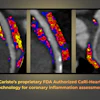
The group recommends using coronary CTA as a prognostic risk tool for stable patients with chest pain while recognizing the technique is lacking in specificity and positive predictive accuracy. These factors led to the development of value-added coronary CTA strategies including fractional flow reserve derived from CT and CT perfusion.
Updated recommendations are listed for evaluating for stable coronary artery disease using the following techniques:
- Coronary CTA in native vessels
- Coronary CTA post revascularization
- Coronary CTA with fractional flow reserve or CT perfusion
- Coronary CTA in other conditions