
Neuroimaging features of hospitalized COVID-19 patients can vary, but they are dominated by altered mental status and acute ischemic stroke, according to a research published May 21 in Radiology.
The findings add to a growing knowledge base of the neurologic manifestations of the disease -- which has been paltry compared with the current understanding of its respiratory effects, according to a team led by Dr. Abdelkader Mahammedi of the University of Cincinnati Medical Center in Ohio.
"Several studies have described the spectrum of chest imaging features of COVID-19," the group wrote. "However, to date, only a few case reports have described COVID-19 associated neuroimaging findings."
Mahammedi's group investigated neurological symptoms and imaging findings in patients with COVID-19 hospitalized in three Italian facilities: the University of Brescia, the University of Eastern Piemonte, Novara, and the University of Sassari.
The study included 725 hospitalized patients with COVID-19 disease confirmed by reverse transcription polymerase chain reaction (RT-PCR) tests between February 29 and April 4. Of these, 108 (15%) had acute neurological symptoms and underwent brain or spine imaging. Most patients (99%) had noncontrast brain CT, while 16% underwent head and neck CT angiography (CTA) and 18% had brain MRI.
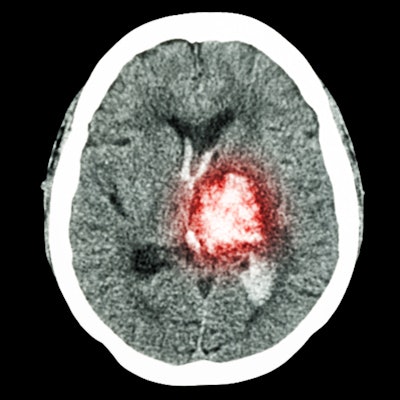
The investigators found that the most common neurological symptoms in patients hospitalized for COVID-19 were altered mental status and ischemic stroke.
| Neurological characteristics of patients hospitalized with COVID-19 | |
| Imaging finding | Percentage of patients (n=108) |
| Altered mental status | 59% |
| Ischemic stroke | 31% |
| Headache | 12% |
| Myalgias | 12% |
| Seizure | 9% |
| Dizziness | 4% |
| Neuralgia | 3% |
| Ataxia | 2% |
| Hyposmia | 2% |
The group also found the following in patients with neurological symptoms at hospital admission:
- 29% had no known past medical history. Of these, a third had acute ischemic stroke and two had intracranial hemorrhage.
- 71% had at least one additional chronic disorder, such as coronary artery disease (23%), cerebrovascular disease (14%), hypertension (51%), or diabetes (28%).
- 66% had no acute findings on CT. Of these, 35% had abnormalities on brain MRI.
The study results show that neuroimaging features of acutely ill patients with COVID-19 are various, according to Mahammedi and colleagues. Although altered mental status and acute ischemic stroke are the most prevalent, radiologists may also find posterior reversible encephalopathy syndrome, hypoxic-ischemic encephalopathy, or a "nonspecific cortical pattern of T2 fluid-attenuated inversion-recovery (FLAIR) hyperintense signal" on MRI, the group wrote.
In any case, the cause of neurological manifestations of COVID-19 needs further research.
"Currently, we have a poor mechanistic understanding of the neurological symptoms in COVID-19 patients, whether these are arising from critical illness or from direct central nervous system invasion of SARS-CoV-2," the researchers concluded. "Accumulating evidence suggests that a subgroup of patients with severe COVID-19 might have a cytokine storm syndrome which could be a trigger for ischemic strokes, probably related to the prothrombotic effect of the inflammatory response."



















