CT helped confirm that the novel coronavirus disease (COVID-19) is indeed capable of triggering moderate-to-severe respiratory illness in otherwise healthy children, despite popular opinion to the contrary, in a study published online March 12 in the New England Journal of Medicine.
The researchers from China, led by Yingle Liu, PhD, from Wuhan University, found that six out of 366 children (1.6%) hospitalized for a respiratory infection from January 7 to 15 within a healthcare network tested positive for COVID-19.
The children were all previously healthy and their median age was 3 years. They presented to the hospital three to five days after the onset of symptoms, with the most common clinical characteristics being high fever, cough, and vomiting. Nucleic acid testing with reverse transcription polymerase chain reaction (RT-PCR) based on throat swab samples confirmed the presence of the coronavirus (SARS-CoV-2) in the pediatric patients.
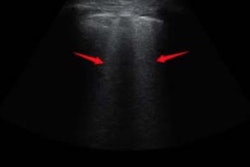
Five of the patients also underwent a chest CT exam. CT showed typical viral pneumonia patterns in four cases, including patchy ground-glass opacities or patchy shadows in both lungs.
Clinicians treated the patients with antiviral agents, antibiotic agents, and supportive therapies. One of the patients was admitted to the pediatric intensive care unit. All of the patients recovered after a median of 7.5 days of hospitalization.
"This study showed that COVID-19 occurred in children, causing moderate-to-severe respiratory illness, in the early phase of the SARS-COV-2 outbreak in Wuhan," the authors wrote.