Dear AuntMinnie Member,
Radiation dose is a major issue for many screening studies, and virtual colonoscopy is no exception. However, unlike another important screening exam -- mammography -- VC practitioners often employ powerful multislice scanners that can pack a radiation wallop if not carefully monitored.
Minimizing dose in virtual colonoscopy is therefore a crucial undertaking -- one that European practitioners in particular have been addressing successfully. Now German researchers have found a potential solution with a technique that modulates x-ray tube current in the z-axis using a 16-slice CT scanner, according to an article by staff writer Eric Barnes that we're featuring this week in our Virtual Colonoscopy Digital Community.
Current dose-modulation protocols vary the radiation dose depending on the attenuation characteristics of the tissue being irradiated. Without such modulation, some organs receive too much radiation and others too little.
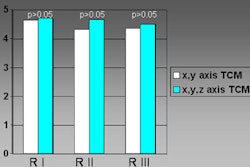
The German group produced good results with their z-axis technique, using updated software that adds a new plane to the existing x- and y-axis modulation. Radiation dose was far lower among patients scanned with the newer protocol, and independent readers found no significant differences in image quality. One can only hope that the bounty of extracolonic abnormalities VC has been finding won't be significantly diminished.
Read all about the study by clicking here. For the rest of the world of virtual colonoscopy, check out our Virtual Colonoscopy Digital Community at vc.auntminnie.com.