When it comes to noninvasive vascular imaging, 16-slice CT angiography (CTA) is far superior to V/Q scans, according to a presenter at the 2003 annual Royal Australian and New Zealand College of Radiology (RANZCR) meeting in Brisbane, Australia.
"What’s better with 16-slice scanning? Everything really," enthused Dr. Ruben Sebben of Jones and Partners’ Medical Imaging in Adelaide, Australia. "Multislice CT angiography has been widely accepted by physicians and surgeons."
Indeed, pulmonary CTA has largely replaced VQ scanning for diagnosing pulmonary embolus, he added. The benefits of 16-slice CTA include significant improvement in detail resolution, reduced radiation dose, faster scans, extended scan distances, and more accurate outcomes, Sebben said.
Because the image voxels are equal in size in all three planes, these isotropic voxels greatly enhance most clinical studies. Multiplanar and 3-D reconstructions demonstrate improved quality because of thinner slices. Enhanced reformation algorithms improve image quality through the reduction of artifacts caused by beam hardening, metal, and heavy calcification. Z-axis resolution of 0.5-1 mm is comparable to digital subtraction angiography resolution, Sebben explained.
Faster scan times reduce the motion artifacts associated with vessel pulsation and swallowing, which is particularly useful for carotid imaging. The current scan time is 0.5 seconds and reconstruction time is 0.5 seconds. Comparisons with conventional angiography consistently show similar diagnostic results, and using CTA can reduce contrast loads, he said.
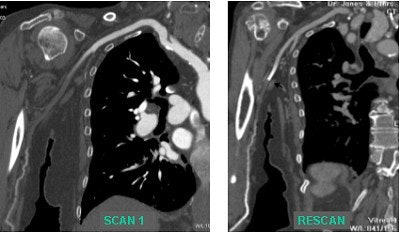
The capability of 16-slice CTA to rescan rapidly enables a second exam to better visualize extremity arterial occlusions, he reported. Improved tibial artery visualization provides very useful presurgical information for potential graft planning.
"The arteries of lower extremity inflow and runoff can be reliably depicted with minimal venous enhancement using multislice CT angiography," Sebben added. In the elderly, vessel tortuosity can be better appreciated, which also facilitates presurgical evaluation, he said. An added bonus of CTA is that it can detect incidental findings in organs.
 |
Clinical cases illustrate the advantages of 16-slice vs. 4-slice and 8-slice imaging. Evaluation using 16-slice imaging enabled vessel visualization over a distance of 1,800 mm, compared with 1,500 mm for 4-slice scanners. This was particularly relevant in the case of a tall man with coexisting carotid and iliac arterial disease. Images courtesy of Dr. Ruben Sebben.
 |
The indications for conventional and multislice CT are the same, such as the evaluation of aorto-bifemoral, thoraco-abdominal, extra- and intra-cranial arteries, and upper limb and hand arteries. Thin-slice pulmonary vasculature, visceral and cardiac vessels, and gastrointestinal bleeding studies can also be assessed. Aneurysms, stenoses, fibromuscular hypersplasias, arterial dissections, subtotal and total occlusions, arterio-venous malformations, vascular stents and grafts, and endoluminal grafts all were well visualized employing 16-slice CTA.
Another advantage of CTA is a lower radiation dose. Sebben referred to a study lead by Dr. Geoffrey Rubin that found conventional angiography exposed patients to 3.9 times more radiation than CTA (Radiology, October 2001, Vol.221:1, pp.146-158).
Sebben noted that CTA does have some disadvantages, including lengthy postprocessing times, generation of large data sets, contraindications to iodinated contrast agents such as allergies and chronic renal failure, and a lack of real-time information.
Sebben suggested that large data sets would prove problematic for long-term storage, and patient radiation dose was still a serious consideration, especially in light of the advent of MR angiography.
However, Sebben predicted that future improvements, such as faster gantry rotation for cardiac imaging, and a reduction in focal spot size for improved image quality, would alleviate some of those issues in CTA. On the computing side, improved processors should result in faster workstation performance, while new software should improve postprocessing capabilities.
"The future is certainly going to see CT angiography continue to evolve," he concluded.
By Leanne McKnoultyAuntMinnie.com contributing writer
January 5, 2004
Related Reading
MDCT finds predictive value in soft plaque, September 24, 2003
Calcium-scoring methods study says it's all good, September 10, 2003
Cardiovascular MRI and MRA, August 21, 2003
Coronary calcium scan gains ground as prognostic tool, August 6, 2003
Copyright © 2004 AuntMinnie.com


















