RECIBM is a new imaging framework that standardizes the evaluation of bone metastases treatment response by integrating multiple imaging modalities, showing strong agreement with existing criteria and improved association with patient survival outcomes.
- RECIBM combines MRI, PET, SPECT, CT, and radiography into a single set of response categories, addressing fragmentation in existing bone metastases assessment frameworks.
- High agreement with established criteria: RECIBM showed kappa values of 0.80 to 0.98 when compared to MD Anderson, PERCIST, and EORTC criteria.
- Reclassified 19% of patients, demonstrating clinically meaningful differences in treatment response interpretation across imaging modalities.
- Superior survival prediction: RECIBM achieved the highest concordance with overall survival (C-index = 0.807) and bone progression-free survival (C-index = 0.849).
- Study included 84 patients with confirmed bone metastases treated between October 2017 and September 2023, with 68% receiving chemotherapy.
A new imaging framework that classifies bone metastases into standardized response categories shows strong agreement with existing response criteria and was associated with patient survival outcomes, according to a study published July 7 in Radiology.
The framework, called the Response Evaluation Criteria in Bone Metastases (RECIBM), synthesizes anatomic and functional imaging and addresses a longstanding gap in how skeletal disease is assessed on treatment, reported lead author Tingting Xu, of Southwest Medical University in Sichuan, China, and colleagues.
“Rather than aiming to establish superiority over existing criteria, RECIBM was designed to address a clinically recognized challenge – discordant interpretation between anatomic and metabolic imaging,” the group wrote.
The principal shortcoming of existing criteria lies in their fragmented nature, the researchers explained, with each framework capturing only one aspect of the multifaceted biologic evolution of bone metastases. To overcome these limitations, the group developed RECIBM through multidisciplinary consensus. The criteria integrate MRI, PET, and SPECT, along with CT and radiography, into a single set of response categories rather than requiring a separate framework for each modality.
In the study, the group evaluated its performance against the MD Anderson (MDA) criteria, the PET Response Criteria in Solid Tumors (PERCIST) criteria, and the European Organization for Research and Treatment of Cancer (EORTC) criteria. The frameworks were applied retrospectively in 84 patients with confirmed bone metastases treated between October 2017 and September 2023. A majority of patients (68%) were receiving chemotherapy.
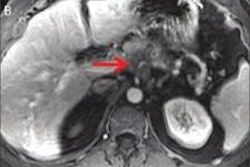
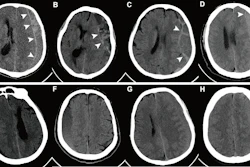
 Response Evaluation Criteria in Bone Metastases (RECIBM) and metabolic criteria were used to detect a complete response missed at anatomic assessment. A 76-year-old male patient presented with 1 month of hemoptysis and was diagnosed with small cell lung cancer and bone metastases. Baseline (July 2022) F-18 FDG-PET/CT images (A, maximum intensity projection image; B–E, axial images) demonstrate FDG-avid lesions in the left lamina of the first lumbar vertebra (L1) (straight yellow arrows; maximum standardized uptake value, 2.74; peak standardized uptake value normalized to lean body mass, 1.59) and left ilium (curved yellow arrows; maximum standardized uptake value, 3.68; peak standardized uptake value normalized to lean body mass, 2.28). After seven chemotherapy cycles (December 2022), follow-up PET/CT images (F, maximum intensity projection image; G–J, axial images) show complete metabolic resolution of bony lesions (L1: maximum standardized uptake value, 1.32, and peak standardized uptake value normalized to lean body mass, 0.85; left ilium: maximum standardized uptake value, 1.48, and peak standardized uptake value normalized to lean body mass, 0.82), without apparent osteolytic or osteoblastic changes at CT. Assessment was stable disease (SD) according to the University of Texas MD Anderson Cancer Center (MDA) criteria but complete response (CR) or complete metabolic response (CMR) according to RECIBM, PET Response Criteria in Solid Tumors (PERCIST), and European Organization for Research and Treatment of Cancer (EORTC) criteria. The patient was alive as of September 30, 2025. RSNA
Response Evaluation Criteria in Bone Metastases (RECIBM) and metabolic criteria were used to detect a complete response missed at anatomic assessment. A 76-year-old male patient presented with 1 month of hemoptysis and was diagnosed with small cell lung cancer and bone metastases. Baseline (July 2022) F-18 FDG-PET/CT images (A, maximum intensity projection image; B–E, axial images) demonstrate FDG-avid lesions in the left lamina of the first lumbar vertebra (L1) (straight yellow arrows; maximum standardized uptake value, 2.74; peak standardized uptake value normalized to lean body mass, 1.59) and left ilium (curved yellow arrows; maximum standardized uptake value, 3.68; peak standardized uptake value normalized to lean body mass, 2.28). After seven chemotherapy cycles (December 2022), follow-up PET/CT images (F, maximum intensity projection image; G–J, axial images) show complete metabolic resolution of bony lesions (L1: maximum standardized uptake value, 1.32, and peak standardized uptake value normalized to lean body mass, 0.85; left ilium: maximum standardized uptake value, 1.48, and peak standardized uptake value normalized to lean body mass, 0.82), without apparent osteolytic or osteoblastic changes at CT. Assessment was stable disease (SD) according to the University of Texas MD Anderson Cancer Center (MDA) criteria but complete response (CR) or complete metabolic response (CMR) according to RECIBM, PET Response Criteria in Solid Tumors (PERCIST), and European Organization for Research and Treatment of Cancer (EORTC) criteria. The patient was alive as of September 30, 2025. RSNA
“RECIBM-defined response classifications showed high agreement with established criteria, reclassified 19% of patients, and were associated with overall survival and bone progression-free survival,” the group wrote.
Ultimately, by addressing discordance between anatomic and functional changes, RECIBM may represent a step toward more integrated response evaluation, the researchers concluded.
In an accompanying editorial, Soheil Mohammadi, MD, of Brigham and Women’s Hospital in Boston, and Ali Guermazi, MD, of Boston University School of Medicine, wrote that the results highlight the promising potential of RECIBM as a standardized, clinically meaningful framework for assessing bone metastases.
“RECIBM occupies a unique niche as the first response assessment framework, to our knowledge, specifically designed for bone metastases that is both modality-agnostic and validated against survival outcomes,” the pair wrote.
An important next step will be determining if RECIBM-guided management improves clinically meaningful outcomes, including overall survival, progression-free survival, quality of life, and avoidance of premature treatment discontinuation due to misinterpretation of flare responses, Mohammadi and Guermazi concluded.
The full study is available here.