Technetium Labeled Cardiac Imaging
Tc-99m-Sestamibi (2-methoxyisobutyl-nitrate) and Tc-99m-Tetrofosmin
Advantages
Technetium agents have the following advantages when compared to thallium:
1- Energy: The 140keV photon is optimal for gamma camera imaging and can produce higher quality images due to less attenuation, less scatter, and a brighter flash within the scintillation detector (Thallium uses low energy Mercury photons [60-83keV] which have high tissue attenuation).
2- Shorter half-life: Technetium has a 6 hour half-life, as opposed to 73 hours for Tl-201. Therefore, one can administer a 10 to 15 times higher dose than thallium which results in a higher count rate [47]. With the use of a larger dose, images can be obtained in a shorter period of time. High count rates also permit the use of gating to assess wall motion and ejection fraction [47].
3- Production: Technetium is available via a generator 24 hours a day. Thallium is cyclotron generated and requires off-site delivery.
Physiology & Pharmacology
Tc-Sestamibi:
Sestamibi is a lipophilic monovalent cation (an isonitrile compound). It enters the cell via passive diffusion across plasma and mitochondrial membranes. It is postulated that MIBI accumulates within the mitochondria and cytoplasm of cells on the basis of electrical potentials generated across the membrane bilayers. At equilibrium it is sequestered largely within mitochondria by a large negative transmembrane potential. The agent is unmetabolized [11] and is fixed intracelluIarly as long as cell membrane integrity is intact and nutrient blood flow persists. It will not be extracted by non-viable myocardium. In plasma, less than 1% of the tracer is protein bound. Prior to use, the radiochemical purity of Tc-Sestamibi should be greater than 90%. Ethanol is the solvent used for quality controlusing paper chromatography. Sestamibi migrates to the top of the strip.
The first pass extraction fraction for Tc-Sestamibi is approximately 65% (lower than that for thallium, which has an extraction fraction of about 85%) [47]. About 1-2% of the injected dose localizes to the myocardium at rest. The lower extraction fraction is overcome by the larger dose of MIBI which results in a higher count rate. Additionally, after initial extraction, blood levels fall rapidly which provides excellent target to background ratios as long as liver and bowel do not interfere with the image.
The uptake of Sestamibi in the myocardium is proportional to blood flow in the physiologic flow range. However, there is a plateau in extraction at higher flow rates, most likely because the tracer enters the cell via diffusion [22,47]. This plateau in extraction occurs at a lower level of increased flow above baseline compared to Tl-201 [47]. Because of the extraction plateau, Tc-sestamibi will underestimate blood flow at high flow rates (>2.0mL/min. per gram or about 2.5-3 times baseline flow [22,47]). Such high flow rates are encountered when using pharmacologic stress agents such as dipyridamole or adenosine. Therefore, it is theoretically possible for a mild to moderate stenosis which does not significantly impair coronary artery flow reserve to be overlooked with sestamibi vasodilator stress imaging [22]. Even so, the higher spatial resolution and lack of redistribution may offset the expected finding of slightly lower defect contrast associated with this reduced extraction at higher flow rates when compared to thallium. Overall, Tc-sestamibi is primarily a perfusion agent- it provides only limited information regarding myocardial viability and will frequently overestimate the amount of myocardial scarring.
Myocardial clearance of Tc-sestamibi is slow and the agent does not redistribute to a degree that can be imaged clinically [16]. Note (the following is certainly beyond what would ever be expected of a radiology resident): Heart House Course, Bethesda '93: Sestamibi undergoes minimal (about 20%) redistribution primarily within the first 20 to 60 minutes following injection. This may impact on lesion detection as the differential washout between the normal and ischemic myocardium may result in a reduction in defect size or severity with time. Therefore, their recommendation was to begin imaging 15 minutes following stress injection, and 60 minutes following rest injection. The tracer is retained in normal myocardium for several hours (myocardial clearance T1/2 is about 5 hours).
The primary route of excretion is hepatobiliary (33%). Clearance via this route is prompt (T1/2 of approximately 30 min.). Unfortunately, scatter from both liver and bowel activity can interference with visualization of the inferior ventricular wall. This activity can be backprojected over the inferior wall during image reconstruction. High hepatic uptake can also create artifactual perfusion defects in the inferior and inferoseptal walls [1]. Finally, this activity may also severely disrupt image normalization programs. There is about 25% renal clearance of the agent. The critical organ is the upper large intestine, which receives about 5.4 rads per 30mCi dose of Sestamibi. Total body dose is about 500mrad.
Tc-MIBI does not concentrate in breast milk to any significant degree and cessation of breast feeding is not necessary following a Tc-MIBI exam. Close contact with the infant, however, should be avoided [17].
Technetium-99m-Tetrofosmin [1,2-bis [bis (2-ethoxyethyl) phosphino] ethane]
Tetrofosmin is a lipophilic, cationic, diphosphine which is rapidly cleared from the blood following intravenous administration [47]. The agent requires only a 15 minute incubation at room temperature for preparation. The agent is taken up by the heart, skeletal muscle, liver, spleen, and kidneys in proportion to blood flow and viability [24]. Between 1 to 1.5% of the injected dose localizes to the myocardium. The uptake mechanism is membrane-potential driven diffusion independent of cation channel transport [24]. The agent accumulates within mitochondria similar to Tc-sestamibi [47]. Myocardial uptake is decreased by metabolic inhibitors that cause severe cell injury or cell death [47].
The agent does not redistribute to any significant degree, but the higher lipophilicity may explain its higher initial uptake and faster washout [24]. The biological half-life for tetrofosmin in normal myocardium is 278 +/- 32 minutes, which is shorter than sestamibi (680 +/- 45 minutes) [24]. Hepatic uptake is lower than with Tc-Sestamibi and it also clears more quickly which can permit imaging sooner after injection (as soon as 5 minutes after exercise injection and 30 minutes for rest injection) [19,20,24].
The mean first pass extraction fraction is about 54% [47]. As with Tc-Sestamibi there is decreased tracer extraction compared to Thallium at high flow rates (such as that encountered with pharmacologic stress). The extraction of Tetrofosmin plateaus at a flow rate of approximately 2.0 mL/min/gm3 (or about 1.5 times normal flow [47]). The heart to lung contrast ratio is similar to sestamibi between 30 to 60 minutes post-injection [24]. Similar to Tc-Sestamibi, lesion conspicuity for mild to moderate stenoses may be less apparent than for Tl201 [47].
Sensitivity & Specificity
The sensitivity/specificity for SPECT Tc-Sestamibi and Tc-Tetrofosmin in the detection of coronary artery disease are almost identical to thallium [2]:
- Sensitivity: About 90%
- Specificity: About 80%
A polar map is available for quantitative analysis of the images. The distance weighted map is best for determining defect location as every ring in the polar map is the same width. The volume weighted map is best for determining defect size (extent and severity), as it makes the 2-dimensional area of a defect equal to its relative 3-dimensional volume. The use of attenuation correction can improve the specificity and normalcy of the exam [53,54].
Same day Rest and Stress study
An initial rest exam followed by the stress study was found to be more effective for determining the presence of reversible abnormalities [3]. A stress/rest sequence results in an increased number of ischemic segments incorrectly being identified as fixed defects (7% false-negatives) [4]. Additionally, in the stress-rest protocol, the rest portion of the exam may not be considered to be a "true" rest study as it follows a period of exercise and this may contribute to the overestimation of scar.
The first injection (rest study) is low dose (8mCi), while the second or stress injection is high dose (22mCi- approximately 3 times the rest dose in order to overwhelm activity remaining in the myocardium) and follows the first by 2-3 hours to permit time for some decay of the agent. Rest images are obtained 1 hour after injection. Some centers have the patients drink 8oz. of whole milk about 15 minutes prior to imaging to promote tracer clearance from the liver and gallbladder. This, however, increases the amount of bowel activity.
Drawbacks of the same day rest-stress protocol are that it provides less than ideal stress defect contrast due to resting background activity. Tc-Sestamibi and Tc-tetrofosmin rest imaging have also been shown to underestimate the extent of viable tissue.
Two-day Stress/Rest Protocol
The 2 day exam provides optimal defect contrast with minimal background activity. Additionally, the rest study would not be necessary if stress study was normal.
Dual Isotope Scanning
In this protocol a rest thallium study (2.5-3.5 mCi) is done first so that there is no interference from scattered technetium photons. If Thallium is injected the day before, images will refect 24 hour redistribution (myocardial viability). Delayed thallium imaging at 24 hours using the dual isotope exam will detect reversible defects in an additional 17% of patients. [5]
A stress Tc-Sestamibi or Tc-Tetrofosmin study is then performed using 20-30 mCi of the agent. No wait is required between the rest and stress study as the Technetium gamma energy is higher than the energy imaged for Thallium. A drawback of this technique is that because of the resolution differences between the two isotopes, it is difficult to directly compare the images, particularly with subtle abnormalities.
Gating- Wall motion and LVEF assessment
Ventricular function data can be assessed by gating during data acquisition. This data can add important prognostic information to the data obtained from the perfusion exam [52].
Wall motion analysis:
Gated planar studies can be used to assess regional wall motion and left ventricular ejection fraction when viewed in a cine display. Gated exams improve the diagnostic accuracy of SPECT imaging by detecting artifacts secondary to soft tissue attenuation. The gated LVEF also provides information regarding myocardial systolic function and prognosis. The study requires performing a gated acquisition during each of the planar projections. Optimally ECG gating is performed using eight to 16 frames for the cardiac cycle. The images obtained for interpretation are sharper than non-gated images and can sometimes increase conspicuity of a perfusion defect. Both wall motion and wall thickening can be evaluated on gated cardiac exams. However, changes in heart rate can result in temporal blurring- in other words- mixing of counts from adjacent frames [51]. To minimize temporal blurring, a beat rejection window is set by specifying the acceptable deviation of each R-R interval from the expected value (a 20% window has historically been applied) [51]. Wall motion is evaluated by measuring the excursion of the ventricular endocardial surface, while wall thickening is evaluated by assessing changes in regional myocardial counts [34]. On gated images wall thickening appears as an increase in myocardial intensity (brightness) from diastole to systole.
If a perfusion defect is present on stress images and the associated wall is seen to thicken (ie: brighten) during systole, one can predict that this represents an area containing viable myocardial tissue. If no thickening is observed, the finding may represent an area of infarction (scar), however, one cannot completely exclude the presence of viable myocardium (hibernating myocardium). If there is insufficient counts from the area of the defect, viable myocardium may not be properly identified even on a gated exam. Hence, areas of hibernating myocardium may be akinetic or dyskinetic with no evidence of thickening, but will recover function following revascularization. False positive gated exams for infarction have also been described in patients with cardiomyopathies and in valvular heart disease in which non-ischemic perfusion defects and wall motion abnormalities may be seen [13].
Gated SPECT during the first hour after exercise is able to assess post-stress cardiac function [26]. Reversible perfusion defects may display post-stress stunning (transient myocardial contractile dysfunction/wall motion abnormality) in areas of ischemia [26]. The incidence and magnitude of regional wall motion abnormalities are related to the severity of ischemia [39]. The time course for resolution of ischemic post-stress wall motion abnormalities can range from immediate to up to 2 hours [32].
In patients with multivessel coronary artery disease, the degree of ischemia can be underestimated because of a relatively balanced global left ventricular hypoperfusion resulting in a normal appearing scan [32]. Post-stress regional wall motion abnormalities detected on the gated exam can be an indicator of severe and extensive coronary disease and provides incremental diagnostic information over perfusion alone [26]. Patients with abnormal wall motion on gated SPECT images have an annual event rate up to 6.1%, compared to 1.6% for patients with normal wall motion [52]
Breast attenuation, diaphragmatic attenuation, and apical thinning can all produce fixed perfusion abnormalities. On gated images, these defects will generally demonstrate normal wall thickening which would not be identified in an area of scarring. Another technical limitation of gated imaging is overestimation of viable myocardium. Approximately 5% of myocardial infarctions are seen to thicken during systole on gated images. This may occur because a small infarct is "pulled in" by adjacent normal myocardium, or the MI may be non-transmural. False positive gated exams for infarction have been described in patients with cardiomyopathies or valvular heart disease in which non-ischemic perfusion defects and wall motion abnormalities may be seen [13].
Abnormal reduced septal motion with normal wall thickening is a common finding on gated SPECT images after coronary artery bypass surgery [34]. This finding is felt to be related to exaggerated systolic anteromedial cardiac translation [34]. As a result of this translocation, lateral wall function is often overestimated [34]. The exaggerated cardiac mobility is thought to be related to sternotomy and pericardiotomy [34].
Ejection fraction:
The cardiac ejection fraction can be calculated from the gated SPECT data and provides incremental prognostic information for risk stratification. There are several software programs which can generate the EF and all have roughly between 70-85% correlation with gated blood pool imaging determined ejection fractions [23]. With serial measurements the calculated LVEF is very reproducible [43] and has a mean variability of about 5% (+/- 3.5%) (higher variability is associated with low count examinations) [38]. In patients with stress induced ischemia, left ventricular function may be temporarily impaired (stunned myocardium) [43]. Global LVEF is generally not impaired until at least 25% of the LV myocardium is ischemic [39]. Global LVEF impairment is also more commonly associated with anterior (LAD) ischemia [39]. In patients with "balanced" multivessel ischemia, an abnormal post-stress LVEF may be the only indication of underlying CAD [51].
Regarding prognostic information, the post-stress ejection fraction is an important determinant for cardiac death [14]. Patients with a post-stress ejection fraction of less than 30% are at an increased risk for cardiac death, regardless of the amount of ischemia identified [14]. Other authors indicate that a post-stress ejection fraction of less than 45% is associated with an elevated risk of major adverse cardiac events [49,51].
Following myocardial infarct: In the early phases following acute MI, left ventricular dysfunction is an independent factor for risk stratification [36]. In the post-MI period, a gated LVEF of less than 40% has been associated with an increased risk for subsequent cardiac event [33]. Generally, the relative risk of death or non-fatal MI doubles for every 10% decrease in LVEF [50].
Unfortunately, early post MI left ventircular function may be impaired [36]. Dysfunctional, but viable, stunned myocardium will gradually return to normal function, and hibernating myocardium will demonstrate improve function following revascularization [36]. Assessment for contractile reserve in areas of hibernating myocardium can be performed using low dose dobutamine (LDD) echocardiography or LDD SPECT imaging (see discussion in Pharmocologic stress imaging section).
Gating errors can affect wall motion analysis and LVEF determination [46]. In patients with arrhythmias, EF fluctuations and wall thickening discordance may occur [51]. With tall T waves, the R-T phase (systole) and the T-R phase (predominantly diastole) are regarded as two cardiac cycles [46]. When the time-volume curve is generated by summation of these phases- which produces essentially a flat line [46]. Repositioning the ECG leads to increase the amplitude of the R wave and decrease the T wave can correct this error [46].
A limitation of software for gated SPECT is overestimation of LVEF [37] and underestimation of LV end-systolic volumes in small ventricles, especially in patients with hyperdynamic LV function (the small heart error). The inaccuracy in measurements is a result of the low spatial resolution (about 15mm) of SPECT imaging which limits effective delineation of the endocardial surface used for LVEF determination [37,51]. This is particularly a problem at end-systole because the LV is at its smallest and the endocardial edges are at their closest points [23]. In fact, the endocardial edges may appear to overlap [23]. Incorrect determination of the position of the edge of the endocardial surface results in an underestimation of end-systolic volume, which results in an overestimation of the LVEF [23]. End-diastolic volume is also markedly underestimated when less than 37 mL [23]. Programs which do not rely on edge detection may provide more accurate LVEF determinations for patients with small ventricles [23]. Arrhythmias do not seem to significantly affect ejection fraction or ventricular volume determinations [25], although other authors state that LVEF determination can be affected by arrhythmias [51].
Ventricular volumes:
Using gated SPECT software the left ventricular end diastolic volume (normal less than 120 mL) can also be calculated and is generally within 15% of the actual end-diastolic volume when the volume is greater than 74 mL [23]. The presence of an increased end-diastolic volume carries additional prognostic information.
LV enlargement significantly increases the mortality rate in patients with acute MI- particularly when there is coexisting myocardial dysfunction [50]. Patients with an LVEF lower than 40% in whom LV expansion develops, have a significantly higher mortality rate compared with those who do not [50].
Exercise First-pass LVEF
Tc-Sestamibi/Tc-Tetrofosmin first pass LVEF determination requires the use of a multicrystal camera. In patients with multivessel disease (particularly 3 vessel disease), the perfusion study may underestimate the severity coronary artery disease (balanced ischemia). These patients, however, often demonstrate a significant drop in LVEF with exercise. A normal exercise LVEF does not exclude the presence of CAD, but it is associated with a better prognosis in patients with CAD. Patients with an abnormal exercise LVEF and known CAD may benefit more from surgical intervention (CABG,PTCA) than from continued medical therapy.
First pass LVEF seems to be the single most important predictor for the risk of cardiac events in patients with known coronary artery disease. An exercise LVEF of 20-40% is associated with a 15% one year cardiac mortality rate, while an exercise LVEF < 20% is associated with a 50% one year cardiac mortality rate.Determination of first pass LVEF in association with pharmacologic stress has not been shown to add clinical information to the perfusion exam [6].
Chamber dilatation with stress
With Sestamibi, stress imaging is delayed 30 to 60 minutes. The left ventricle (LV) is unlikely to still be transiently dilated due to ischemia. If LV chamber dilatation is noted, it is most likely a reflection of diffuse subendocardial ischemia and multivessel coronary artery disease, rather than true cavity dilatation. Left ventricular chamber dilatation may also be noted with pharmacologic stress and is associated with an increased risk for subsequent cardiac event [10] (again, I suspect this represents subendocardial ischemia or diffuse reduced subendocardial flow reserve).
A planar LAO image immediately following exercise can be performed to assess true chamber size. If LV dilatation is present, there is a high association with multivessel CAD and high grade stenoses.
|
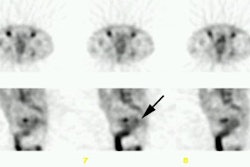
Multivessel coronary artery disease: The patient below underwent Tc-myoview SPECT imaging following pharmacologic stress with adenosine. Short axis images revealed a partially reversible inferior wall perfusion abnormality and a small fixed apical defect, but the significant finding was left ventricular chamber dilatation with stress. This finding is often indicative of multivessel coronary artery disease. At cardiac catheterization, the patient was shown to have three vessel disease. Their gated post stress left ventricular ejection fraction was also decreased (LVEF=41%). (Click image to view all slices) |
|
|
Pulmonary activity on stress imaging
An increase in Tc-sestamibi lung uptake on stress imaging is a marker for severe underlying coronary artery disease [29]. A lung to heart ratio of greater than 0.33 is suggestive of underlying severe CAD [29].
Prognostic Value:
Patients with acute chest pain
In the evaluation of patients with chest pain of suspected cardiac origin, but no ECG evidence of cardiac ischemia, Tc-Sestamibi and Tc-Myoview imaging may also provide diagnostic and prognostic information [18,27]. Additionally, using a normal myocardial perfusion exam as a criterion NOT to admit patients can reduce total admissions and result in substantial cost savings [27,35]. Perfusion imaging in the acute setting is most useful in those patients with no history of prior MI or underlying cardiac disease [48].
Patients injected in the ER, with evidence of a perfusion defect on the MIBI scan were found to have coronary artery disease or a myocardial infarction in nearly 100% of the cases (there were 3 false positive studies). On the other hand, patients with a negative MIBI scan had no cardiac events up to 18 months after discharge. Additionally, based upon catheterization or myocardial perfusion stress exam, no patient with a negative exam was determined to have coronary artery disease [9]. Based upon this data, patients could be risk stratified regarding their risk for actual cardiac event and potentially discharged- thereby avoiding a costly hospital admission [10]. Unfortunately, it is obvious that this technique will be less useful in patients with a history of prior MI in whom perfusion defects can be anticipated [18].
Tc-Myoview has also been used in this setting [27]. The exam has a sensitivity of 90% for acute myocardial infarction [27]. Patients with definitely normal exams have a very low cardiac event rate both during the hospital period and during short-term follow-up, with a high negative predictive value of 99% [27]. Unfortunately, many patients do have abnormalities on their studies which decreases the specificity (60%) and the positive predictive value (12%) [27]. Between 2-5% of patients with normal scans may have underlying coronary artery disease that will require revascularization and further outpatient evaluation will be required in select patients [27].
Imaging the Acute MI
The purpose of reperfusion therapy in patients with acute myocardial infacrtion is to achieve significant myocardial salvage and to limit the extent of irreversible tissue damage [20]. Salvaged myocardium is defined as the the difference between the initial area at risk and the final infarct size. Even a satisfactory angiographic result after PTCA does not always imply effective tissue reperfusion with consequent myocardial salvage [20]. Technetium based perfusion agents such as Sestamibi or Tetrofosmin can be injected in the emergency room to patients experiencing acute myocardial infarction. After initiation of reperfusion therapy and stabilization, images can be obtained which represent the extent of myocardium at risk at the time of infarction [50]. Subsequent images performed prior to discharge can be compared to the original exam and can assess the degree of myocardial salvage and viability [7,21].
There is excellent correlation between the size of histologic infarction and the measured region of absent perfusion on tomographic images. The absolute minimal activity (ie: the lowest pixel count) within an area of infarction, is strongly predictive of the eventual infarct size and the presence or absence of collateral flow. Although correlation with viability is reasonably high in the setting of acute infarction, cellular myocardial function does not immediately return to normal following revascularization and follow-up exams should be delayed for a period of time prior to reimaging [21]. Sestamibi uptake may not return to normal for up to 14 days following MI, reflecting metabolic derangements of tracer uptake or persistent microvascular dysfunction which limits the return of flow. The amount of salvaged myocardium is typically completely demonstrated by 7 days following revascularization on Tc-tetrofosmin imaging [21].
Drawbacks of imaging patients with acute infarction are the technical and logistical difficulties of imaging patients in the acute setting, the limited availability of imaging after normal hours, and agent preparation times- Sestamibi requires 30 minutes to prepare the dose and has a shelf life of only 6 hours (which would require preparation 4 times a day to have the dose routinely available on an emergent basis).
Another important factor in the evaluation of patients following emergent reperfusion for acute infarction is the resultant left ventricular ejection fraction (LVEF) [20]. Unfortunately, gated SPECT ejection fraction may not be accurate in the immediate post infarct period due to post-ischemic stunning and persistent contractile dysfunction [20]. The demonstration of contractile reserve within asynergic segments using dobutamine echocardiography (inotropic stimulation) can identify viable, but "stunned" myocardium [20]. The detection of any contractile reserve (even minimal wall motion) in the infarcted zone is an accurate predictor of increased LVEF during late follow-up [20].
Imaging in the early post-infarct period:
In the post-infarct period, patients with evidence of ischemia on myocardial perfusion imaging have a significantly higher risk for subsequent cardiac events compared to patients without ischemia [42]. The greater the extent of ischemia, the more likely patients are to have a subsequent event [42,50]. Gated LVEF determination also provides prognostic information. Patients with post-infarct LVEF's less than 40% have a 3 fold increased risk for cardiac death or infarction [42]. Even with submaximal exercise, SPECT imaging is more likely to demonstrate regions of ischemia compared to ECG findings alone [50]. Pharmacologic stress imaging can also be employed as early as one to two days following acute myocardial infarction allowing very early risk stratification [50]. With pharmacologic stress, patients with small (less than 10%) or predominantly nonischemic defects can generally be treated conservatively, while patients with more extensive ischemia should be managed more aggressively due to their higher risk for subsequent cardiac event [50].
Patients with known or suspected CAD
Technetium agent myocardial perfusion imaging yields incremental prognostic information towards the identification of patients at risk for cardiac events [15]. Patients with adequate exercise stress and a normal Sestamibi exam have an overall annualized cardiac event (MI or cardiac death) rate of less than 0.5-2% per year [8,10,15,41,44]. From a multicenter registry, the annualized cardiac death rate for patients with a normal tetrofosmin exam has also been shown to be very low (0.6%) [40]. However, even if the perfusion scan is normal, it has been demonstrated that the cardiac death or non-fatal infarction rate is higher in patients with previously document coronary artery disease [44] (about 2% per year [49]). Other factors associated with a higher risk for events, despite a normal perfusion scan include pharmacologic stress, diabetes mellitus, males gender, and increasing age [44,49,52]. Thus, in specific patient populations, close follow-up may be warranted with serial testing in as early as one year [49].
Conversely, an abnormal Sestamibi exam which demonstrates a reversible defect is associated with a significantly increased risk for cardiac events [10]. An increased number of reversible defects, the presence of defects in multiple vascular territories, and the severity and extent of reversible defects are all associated with an increased risk for subsequent cardiac event [10,14,52]. The most severe reversible perfusion defect does not necessarily reflect the cardiac territory at greatest risk for subsequent infacrtion [12]. Severe stenoses are more likely to be associated with collateral circulation and infarction is more likely to complicate acute thrombosis of a mildly obstructive plaque [12].
The results of the myocardial perfusion exam can also aid in risk stratification and provide a guide for the most effective treatment options [15]. In patients with severely abnormal scans indicating extensive ischemia, early revascularization will result in a decreased rate of cardiac death compared to a similar group of patients treated with medical therapy [15]. Patients with mildly abnormal exams have a greater risk for myocardial infarction, rather than cardiac death, and this subgroup of patients would likely benefit most from initial initial treatment [15]. Referral to catheterization and the accompanying costs may not be required if symptoms can be controlled with medical therapy [15].
In general, patients with prior MI that are more likely to have a cardiac event tend to be more symptomatic, are more frequently diabetic, and are more likely to undergo adenosine stress imaging [31]. However, cardiac event rates have also been shown to increase as a function of SPECT abnormalities [31]. Very low event rates of less than 1% are observed in patients with small MI's and no or only mild ischemia [31]. Patients with moderate or severe ischemia, and patients with large MI's had a greater likelihood of having cardiac events [31].
Following angioplasty and stent placement in patients without myocardial infarction and following coronary artery bypass grafting:
Reversible perfusion defects can be found in 30-50% of patients following coronary balloon angioplasty and the finding is associated with a high risk of restensosis [28]. In spite of a good angiographic appearance, intravascular ultrasound has shown that some of the reversible perfusion abnormalities can be explained by an inadequate result [28]. Other etiologies which may explain reversible perfusion abnormalities in post-angioplasty patients include a transient defect in distal vessel autoregulation or a local spasm of the vessel wall at the site of dilatation [28].
Following coronary stent placement, reversible perfusion abnormalities can be found in up to 17% of patients and the finding is also associated with an increased risk for restenosis [28]. The reversible perfusion abonrmalities may be related to impairment of the microvascular response to stress, microvascular stunning due to particulate embolization associated with the procedure, unapparent angiograhpic obstruction at or adjacent to the stent (unapparent stent-edge dissection or new accumulations of focally extruded plaque) or unrecognized incomplete stent expansion [28].
In patients that have undergone revascularization with either percutaneous intervention or CABG, the presence of reversible perfusion abnormalities is associated with a significantly increased risk for subsequent cardiac events- even in asymptomatic patients [45]. A normal study in this same cohort, is associated with a very low risk for cardiac events [45].
Evaluation of Myocardial Viability
See Myocardial Viability in the Thallium section
REFERENCES:
(1) J Nucl Med 1994; Germano G, et al. A quantitative phantom analysis of artifacts due to
hepatic activity in technetium-99m myocardial perfusion SPECT studies. 35: 356-59
(2) Am J Cardiology 1990; Maddahi J, et al. Myocardial perfusion imaging with technetium-99m sestamibi SPECT in the evaluation of coronary artery disease. 66: 55E-62E
(3) Eur J Nucl Med 1988; Taillefer et al. Myocardial perfusion imaging with 99mTc-methoxy-isobutyl-isonitrile (MIBI): comparison of short and long time intervals between rest and stress injections. Preliminary results. 13: 515-522
(4) Radiol Clin North Am 1993; Borges-Neto S, Coleman RE. Radionuclide ventricular function analysis.31: 817-830
(5) J Nucl Med 1994; Kiat H, et al. Comparative feasibility of separate or simultaneous rest thallium-201/stress technetium-99m-sestamibi dual-isotope myocardial perfusion SPECT. 35: 542-48
(6) J Nucl Med 1994; Sciagra R, et al. Evaluation of coronary artery disease using technetium-99m-sestamibi first-pass and perfusion imaging with dipyridamole infusion. 35: 1254-64
(7) J Nucl Med 1992; Gibson WS, et al. Serial tomographic imaging with technetium-99m-sestamibi for the assessment of infarct-related arterial patency following reperfusion therapy. 33: 2080-85
(8) J Nucl Med 1994; Brown KA, et al. Prognostic value of normal technetium-99m-sestamibi cardiac imaging. 35: 554-57
(9) J Am Coll Cardiol 1993; Varetto T, et al. Emergency room technetium-99m sestamibi imaging to rule out acute myocardial ischemic events in patients with nondiagnostic electrocardiograms. 22: 1804-8
(10) Chest 1999; Mandalapu BP, et al. Technetium Tc 99m Sestamibi myocardial perfusion imaging. Current role for evaluation of prognosis. 115: 1684-1694
(11) J Nucl Med 2000; Walicka MA, et al. Morphological transformation of C3H 10T1/2 cells by 99mTc-Cardiolite. 41: 1545-1551
(12) J Nucl Med 2001; Candell-Riera J, et al. Relationship between the location of the most severe myocardial perfusion defects, the most severe coronary artery stenosis, and the site of subsequent myocardial infarction. 42: 558-563
(13) J Nucl Med 1995; June; p.952-55
(14) J Nucl Med 2001; Sharir T, et al. Prediction of myocardial infarction versus cardiac death by gated myocardial perfusion SPECT: Risk stratification by the amount of stress-induced ischemia and the poststress ejection fraction. 42: 831-837
(15) Ciculation 1998; Hachamovitch R, et al. Incremental prognostic value of myocardial perfusion single photon emission computed tomography for the prediction of cardiac death. Differential stratification for risk of cardiac death and myocardial infarction. 97: 535-543
(16) J Nucl Med 1993; Villanueva-Meyer J, et al. Assessment of myocardial perfusion defect size after early and delayed SPECT imaging with technetium-99m-hexakis 2-methoxyisobutyl isonitrile after stress. 34: 187-192
(17) Eur J Nucl Med 1994; Klopper RS, et al. The excretion of radiopharmaceuticals in human breast milk: Additional data and dosimetry. 21: 144-153
(18) Semin Nucl Med 1995; Newhouse HK, Wexler JP. Myocardial perfusion imaging for evaluating interventions in coronary artery disease. 25: 15-27
(19) J Nucl Med 1995; Mahmood S, et al. Combined rest thallium-201/stress technetium-99m-tetrofosmin SPECT: feasibility and diagnostic accuracy of a 90-minute protocol. 36: 932-935
(20) J Nucl Med 1995; Cuocolo A, et al. Technetium-99m-tetrofosmin regional myocardial uptake at rest: relation to severity of coronary artery stenosis in previous myocardial infarction. 36: 907-13
(21) J Nucl Med 2001; Tanaka R, Nakamura T. Time course evaluation of myocardial perfusion after reperfusion therapy by 99mTc-tetrofosmin SPECT in patients with acute myocardial infarction. 42: 1351-1358
(22) J Nucl Med 2001; Taki J, et al. 99mTc-sestamibi retention characteristics during pharmacologic hyperemia in human myocardium: comparison with coronary flow reserve measured by doppler flowire. 42: 1457-1463
(23) J Nucl Med 2001; Nakajima K, et al. Accuracy of ventricular volume and ejection fraction measured by gated myocardial SPECT: Comparison of 4 software programs. 42: 1571-1578
(24) J Nucl Med 1997; Munch G, et al. Myocardial technetium-99m-tetrofosmin and technetium-99m-sestamibi kinetics in normal subjects and patients with coronary artery disease. 38: 428-432
(25) J Nucl Med 1999; Nichols K, et al. Influence of arrhythmias on gated SPECT myocardial perfusion and function quantification. 40: 924-934
(26) J Nucl Med 2001; Sharir T, et al. Quantitative analysis of regional motion and thickening by gated myocardial perfusion SPECT: Normal heterogeneity and criteria for abnormality. 42: 1630-1638
(27) J Am Coll CArdiol 1998; Heller GV, et al. Clinical value of acute rest technetium-99m tetrofosmin tomographic myocardial perfusion imaging in patients with acute chest pain and nondiagnostic electrocardiograms. 31: 1011-17
(28) J Nucl med 2001; Rodes-Cabau J, et al. Frequency and clinical significance of myocardial ischemia detected early after coronary stent placement.
(29) J Nucl Cardiol 2001; Choy JB, Leslie WD. Clinical correlates of Tc-99m sestamibi lung uptake. 8: 639-44
(30) J Nucl Med 2002; Sciagra R, et al. Comparison of dobutamine echocardiography and 99mTc-sestamibi tomography for prediction of left ventricular outcome after acute myocardial infarction treated with successful primary coronary angioplasty. 43: 8-14
(31) J Nucl Cardiol 2002; Zellweger MJ, et al. Risk stratification in patients with remote prior myocardial infarction using rest-stress myocardial perfusion SPECT: prognostic value and impact on referral to early catheterization. 9: 23-32
(32) J Nucl Med 2002; Shirai N, et al. Incremental value of assessment of regional wall motion for detection of multivessel coronary artery disease in exercise 201Tl gated myocardial perfusion imaging. 43: 443-450
(33) Am J Cardiol 2001; Kroll D, et al. Prognostic value of stress-gated Tc-99m sestamibi SPECT after acute myocardial infarction. 87: 381-86
(34) J Nucl Med 2002; Taki J, et al. Electrocardiographic gated 99mTc-MIBI SPECT for functional assessment of patients after coronary artery bypass surgery: comparison of wall thickening and wall motion analysis. 43: 589-595
(35) J Nucl Cardiol 2002; Knott JC, et al. Impact of acute chest pain Tc-99m sestamibi myocardial perfusion imaging on clinical management. 9: 257-262
(36) J Nucl Cardiol 2002; Simones MV, et al. Prediction of left ventricular wall motion recovery after acute myocardial infarction by Tl-201 gated SPECT: incremental value of integrated contractile reserve assessment. 9: 294-303
(37) J Nucl Med 2002; Feng B, et al. Calculation of the left ventricular ejection fraction without edge detection: application to small hearts. 43: 786-794
(38) J Nucl Cardiol 2002; Vallejo E, et al. Variability of serial same-day left ventricular ejection fraction using quantitative SPECT. 9: 377-84
(39) J Nucl Cardiol 2002; Paul AK, et al. Characteristics of regional myocardial stunning after exercise in gated myocardial SPECT. 9: 388-394
(40) J Nucl Med 2003; Shaw LJ, et al. Prognostic value of normal exercise and adenosine 99mTc-tetrofosmin SPECT imaging results from the multicenter registry of 4,728 patients. 44: 134-139
(41) J Nucl Cardiol 2003; Elhendy A, et al. Long-term prognosis after a normal exercise stress Tc-99m sestamibi SPECT study. 10: 261-266
(42) J Nucl Med 2003; Spinelli L, et al. Prognostic value of combined assessment of regional left ventricular function and myocardial perfusion by dopamine and rest gated SPECT in patients with uncomplicated acute myocardial infarction. 44: 1023-1029
(43) J Nucl Cardiol 2003; Verberne HJ, et al. Stress-related variations in left ventricular function as assessed with gated myocardial perfusion SPECT. 10: 456-463
(44) J Nucl Cardiol 2003; Beller GA. Clinical value of myocardial perfusion imaging in coronary artery disease. 10: 529-542
(45) J Nucl Cardiol 2003; Elhendy A, et al. Risk stratification of patients after myocardial revascularization by stress Tc-99m tetrofosmin myocardial perfusion tomography. 10: 615-622
(46) J Nucl Cardiol 2003; Kasai T, et al. Impact of gating errors with electrocardiography gated myocardial perfusion SPECT. 10: 709-711
(47) J Nucl Cardiol 2004; Beller GA, Bergmann SR. Myocardial perfusion imaging agents: SPECT and PET. 11: 71-86
(48) J Nucl Cardiol 2004; Allman KC, Freedman SB. Emergency department assessment of patients with acute chest pain: myocardial perfusion imaging, blood tests, or both? 11: 87-89
(49) J Nucl Cardiol 2004; Shaw LJ, Iskandrian AE. Prognostic value of gated myocardial perfusion SPECT. 11: 171-185
(50) J Nucl Cardiol 2004; Mahmarian JJ, et al. Role of nuclear cardiac imaging in myocardial infarction: postinfarction risk stratification. 11: 186-209
(51) J Nucl Med 2004; Go V, et al. The diagnostic and prognostic value of ECG-gated SPECT myocardial perfusion imaging. 45: 912-921
(52) J Nucl Cardiol 2004; Travin MI, et al. The prognostic value of ECG-gated SPECT imaging in patients undergoing stress Tc-99m sestamibi myocardial perfusion imaging. 11: 253-262
(53) J Nucl Cardiol 2004; Grossman G, et al. Quantitative Tc-99m sestamibi attenuation-corrected SPECT: development and multicenter trial validation of myocardial perfusion stress gender-independent normal database in an obese population. 11: 263-272
(54) J Nucl Cardiol 2004; Heller GV, et al. Clinical value of attenuation correction in stress-only Tc-99m sestamibi SPECT imaging. 11: 273-81