The subject of coronary artery calcium (CAC) screening technology, specifically the suitability of electron-beam CT (EBCT) vs. spiral CT, has stirred deep controversies that only research will be able to quell.
For example, while previous reports have shown significant interscan variability in CAC scores obtained with EBCT, there has been little research on the accuracy, and even less on the reproducibility, of CAC scoring with spiral CT.
A group from Johns Hopkins University in Baltimore contributed significantly to the knowledge in this area in a presentation Wednesday at the RSNA meeting. The researchers found high reliability and reproducibility of scores obtained with a Volume Zoom IV 4x4 multislice scanner (Siemens Medical Solutions, Iselin, NJ).
To be sure, image acquisition times with all technologies are still substantially slower than the cardiac cycle at about 40 ms, resulting in motion artifacts that nibble at the reliability of results. But significant improvements in single-detector spiral CT technology have brought acquisition times down to 500 ms or lower -- 250 ms and lower using partial volume reconstruction techniques. Not quite as fast as EBCT, but pretty close.
For a variety of reasons, then, the latest MDCT scanners might do an even better job, Here, the inter-observer results could be instructive, and the reproducibility of the results could be key.
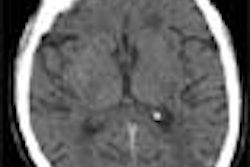
"It is said that a gentleman or a lady with one watch knows what time it is, but a person with two watches is never sure," said presenter Dr. Leo Lawler from Johns Hopkins University. "If the two watches say the same time it's obviously a lot more reassuring, so we decided to look at the reliability and reliability and reproducibility of MDCT for calcium scoring at our institution. Of course, we're talking about measuring the high-density values above the Hounsfield units (HU) of the muscle in the heart, and assuming that's coronary artery calcification within reach of the vessels."
The study looked at 75 asymptomatic patients routinely referred for CAC scoring. Two sets of prospectively gated studies (diastolic phase) were acquired on the same day for each patient using the Siemens scanner with an adaptive array design. Continuous images were acquired with detector collimation of 3 x 2.5 mm in 2.5-mm slice sequential scanning mode, with partial volume reconstruction performed on a Siemens 3-D Virtuoso workstation. The entire 120-mm z-axis sequence coverage, from the carina to the base of the heart, took approximately 18 seconds at 20-40 mAs. Temporal resolution was 250 ms with partial volume reconstruction.
Two sets of scores were acquired. Total scores were examined rather than individual vessels, and results were divided into discrete and continuous data categories.
The total calcium scores ranged from 0 to 2,498 HU, and the average inter-observer difference was 20 HU with a range of 0 to 288.
"We find for discrete data for an individual ... there were 12 times when they saw calcium in one scan and did not see it in the other one," Lawler said. "Only on one occasion was the value rated as zero on one scan higher than 10 on a second scan... For between readers for discrete data ... there were 34 times where one reader saw calcium and the others did not."
Moreover, the mean difference between the first and second scan was 25 HU, with a range from 0 to 473. Most of the large differences between observers were concentrated in differentiating aortic wall, left main artery calcifications and beam hardening artifact, and not the detection of calcification itself.
"When we looked between the scans on continuous data, we found that there was variability greater than 50 for the first reader 12 times, the second reader 11 times, the third reader 7 times…. Most of the scores where people differed, they were already pretty large scores," he said. The significance of that result depends on the model of therapy; a threshold model in which therapy begins at greater than 300 or 350 HU would not be affected by variability at the high end.
In a comparison of the concordance of readers in discrete data, .75 is considered to be a good score for a reliable clinical test, and all of the readers scored higher than .9. The results of 2 types of correlation coefficients calculated for the continuous data, that is, the individual scores, also exceeded .9 for each reader.
"Again, people were very reliable and [the results] reproducible in detecting calcium, and in terms of the actual scores that were assigned," Lawler said. "The second scan [yielded] similar kinds of numbers."
There was a high degree of correlation both within and between readers, though as might be expected, the intra-reader variability was a little less than interreader variability, Lawler said. Moreover, there is reproducibility in detecting calcium in the sense that when it's missed it's a very small value, and when it's present the readers were pretty good at finding it, with reasonably similar scores.
"At our institution, we think MDCT is reliable and reproducible. If one scan is zero the probability of the second scan varying significantly is low.... And it was not useful in our study to have a reader read it more than once, or to have multiple readers read a scan."
By Eric Barnes
AuntMinnie.com staff writer
November 28, 2001
For the rest of our coverage of the 2001 RSNA meeting, go to our RADCast@RSNA 2001.
Copyright © 2001 AuntMinnie.com