Dear AuntMinnie Member,
It was a big week for the CT community. On Thursday, the U.S. Centers for Medicare and Medicaid Services (CMS) issued its final approval of an expansion in coverage for CT lung cancer screening exams.
The news wasn't unexpected -- CMS indicated in November 2021 that it would expand its payment policies, in line with broader screening guidelines issued by the U.S. Preventive Services Task Force early in 2021. The new policies support CT lung screening at age 50 -- five years younger than the previous guidelines -- and reduce the required smoking history from 30 pack years to 20 pack years.
Hopefully, both policies will bolster what has been up to now anemic uptake of lung screening compared with other types of screening exams.
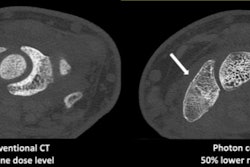
In other news, an article on a new CT technology called dark-field CT was our top story of the week. And researchers from Switzerland found that artificial intelligence (AI) was able to identify intracranial hemorrhage on CT while also improving workflow in the emergency department.
Other important stories of the week covered the following issues:
- Patient stress and anxiety can lead to repeated MRI scans.
- Loneliness can increase the risk of dementia threefold -- a phenomenon visible on brain MRI.
- Recent advances in AI technology are raising medicolegal issues.
- Women shouldn't delay screening mammograms over concerns about lymphadenopathy after getting vaccinated for COVID-19.
Thanks to the hundreds of radiology professionals who tuned in to our webinar on AI for neuroradiology on Thursday! It was a great discussion, and thanks also to our panelists, Dr. Marion Smits, Dr. Alexander Radbruch, and Dr. Peter Chang. Don't worry if you missed it; you can watch it on demand at your leisure.