
Screening-detected breast cancers lead to better overall outcomes over clinically detected cancers, according to research published June 18 in the American Journal of Roentgenology.
A team led by Steven Chen, MD, from State University of New York at Stony Brook University Hospital, found that breast cancers detected via screening mammography were tied to smaller tumor size, earlier stage of diagnosis, less-invasive therapies, and improved overall survival.
“The findings provide evidence supporting screening mammography and indicate the importance of inclusion of the method of detection in registries and other prospective data collections,” the Chen team wrote.
The debate continues as to when and how often women should be screened for breast cancer, with imaging societies and governing bodies having varying guidelines. Recent studies suggest that women should begin undergoing screening mammography at age 40, owing to better prognoses for cancers found early in women ages 40 to 49.
Chen and colleagues suggested that one contributor to these varying guidelines is limited research assessing associations between how breast cancers are found and cancer outcomes. The researchers compared tumor characteristics, treatments, and survival outcomes between women with breast cancer detected by screening mammography versus detection by clinical symptoms.
The retrospective study included data collected between 2010 and 2020 for women with biopsy-proven breast cancer. The team used propensity-score matching between the screening-detected and clinically detected cohorts by age, race, ethnicity, insurance status, and year of diagnosis.
Before propensity-score matching, the data included 1,460 women with breast cancer, of whom 932 had their cancers found through screening and 528 had their cancers clinically detected. After matching, the final analysis included 507 patients in both cohorts.
The researchers reported the following:
Tumor size measured 1 mm to 10 mm in 42% of screening-detected cancers versus in 13% of clinically detected cancers (p < 0.001).
Compared to clinical detection, screening detection led to significantly better five-year (94.4% vs. 79.6%, p < 0.001) and 10-year survival rates (82.7% vs. 66.1%, p < 0.001).
Also, the frequencies of disease types and surgical therapy methods varied between the two cohorts.
Comparison between disease type and treatment methods by cohort | ||
Disease/treatment method | Clinical detection | Screening detection |
Non-invasive disease | 8.9% | 35.5% |
Localized disease | 47.3% | 54% |
Regional disease | 34.1% | 9.9% |
Distant metastatic disease | 7.7% | 0% |
Lumpectomy | 39.3% | 66.1% |
Mastectomy | 34.3% | 22.1% |
Radiation therapy | 41.2% | 50.1% |
Chemotherapy | 40.2% | 15% |
| *All data achieved statistical significance. | ||
Finally, the team noted disparities in its study. Women with screening-detected cancers were more often white and had private insurance, while women with clinically detected cancers were more often Hispanic or Latino and insured by Medicaid.
The results support professional society recommendations for screening mammography and inclusion of detection methods in registries and other prospective forms of data collection, the study authors highlighted.
“Overall survival was significantly greater in the screening-detected cohort than in the clinically detected cohort, providing strong evidence supporting mammographic screening,” they wrote.
The full study can be accessed here.




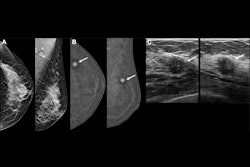








![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)



