Historically, the prospect of reading elbow MR images may have had radiologists burying their heads in their hands.
"It used to be that, before the advent of PACS, MRI of the elbow was relatively straightforward," joked Dr. Garry Gold at the June "MR Advances in Musculoskeletal Imaging and Neuroradiology" conference sponsored by Stanford University of Stanford, CA. "You found one in the 'in' slot in the reading room, and then you found a place to hide it."
"With PACS, (the scans) are a lot harder to hide," added Gold, an assistant professor of radiology at Stanford.
Perhaps radiologists have been seeking to avoid several pitfalls in MR imaging of the elbow as highlighted by Gold in his presentation, including:
Pseudodefect of the capitellum
"This occurs because the capitellum is not a smooth, articular surface across its entire structure," Gold noted. "Only a portion of this is covered by cartilage. As you get more posterior, the capitellum becomes rough and irregular and not part of the articulation."
"The pitfall is that on the coronal image, when you look at the scan, you see the radial head and you see a very irregular-appearing capitellum," Gold said. "You can call that an osteochondritis dissecans of the capitellum, but the truth is that it's just a normal part of the anatomy."
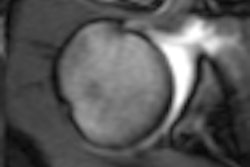
Trochlear notch
The trochlear notch, pictured above, comes from the fusion of the ossification centers for the olecranon and the capitellum on the ulnar, and is a bony ridge that lies between the cartilage covering the olecranon and the cartilage covering the capitellum. However, Gold noted: "This is a normal anatomic variant. This is not an area of damage."
Fat pads and synovial folds
"Synovial folds and fat pads can often have unusual appearances," Gold said. "At some point, you might be concerned with synovitis. Often times, normal synovial folds will give this appearance."
"When you are looking at an elbow, you are going to look for the common injuries," Gold said, outlining several, including lateral epicondylitis, or tennis elbow, an overuse injury that occurs when the common extensor tendon is degenerated and torn. MR is useful for assessing the degree of tendon damage, as well as ruptures of the lateral collateral ligament complex, Gold noted.
Other common injuries include golfer's elbow, or medial epicondylitis, which is related to overuse of the common flexor/pronator muscle group. And athletes who regularly throw, such as pitchers, can be devastated by an injury to the medial collateral ligament, Gold noted, as well as tears in the ulnar collateral ligament that may only have been seen by an MRI.
For optimal MR imaging of the elbow, Gold recommended the following:
- Use of a combination of T1-weighted, proton density, and T2-weighted sequences in all three planes;
- A coronal gradient-recalled echo scan to examine articular cartilage;
- High-matrix imaging (512 x 256), small field-of-view (10-12 cm), and short echo trains (6-8);
- Inclusion of radial tuberosity in the field-of-view of all imaging planes; and
- Imaging with the axial plane perpendicular to the shaft of the humerus.
Finally, "the ideal position has the arm or hand raised with the arm extended over the head, which allows you to put the arm closer to the center of the scanner," he said.
"Some patients will find that position uncomfortable. If that's the case, a supine position with the arm at the side minimizes patient motion," Gold said.
By Shalmali Pal
AuntMinnie.com staff writer
August 14, 2000
Let AuntMinnie.com know what you think about this story.
Copyright © 2000 AuntMinnie.com