FDG-PET imaging has shown for the first time that prednisolone is a potent therapeutic tool for patients with active cardiac sarcoidosis, according to a recent study in JACC: Cardiovascular Imaging.
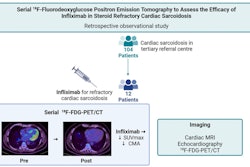
A group led by cardiologist Ryota Morimoto MD, PhD, of Nagoya University in Japan, performed F-18 FDG PET scans in patients before and after a six-month regimen of prednisolone, and the imaging revealed that patients responded to the treatment.
"The current study found high efficacy of [prednisolone] and reconfirmed that it is a first-line drug of choice in the treatment of cardiac sarcoidosis with active inflammation in the heart," the group wrote.
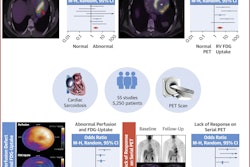
In cardiac sarcoidosis, immune cells form tiny clusters in heart tissue that interfere with normal functioning. This can cause arrhythmias and lead to cardiomyopathy or heart failure. In previous studies, FDG-PET has shown promise for detecting cardiac sarcoidosis based on abnormal uptake of the FDG radiotracer by heart muscle cells, the authors explained.
Although prednisolone is considered a first-line drug for the treatment of cardiac sarcoidosis, neither it nor other immunosuppressive drugs in patients intolerant to prednisolone have been tested in randomized clinical trials, the authors noted.
To address this knowledge gap, the group aimed to evaluate the efficacy of prednisolone in patients with cardiac sarcoidosis and active myocardial inflammation using F-18 FDG-PET. In addition, because methotrexate is frequently used in patients who are intolerant to prednisolone, they also investigated its efficacy.
The researchers recruited 59 patients with active cardiac sarcoidosis and performed PET scans before and after a six-month regimen of prednisolone. Poor responders were randomly assigned to receive methotrexate or repeat prednisolone for another six months and were then also assessed. To determine the effects of the drugs, the researchers used FDG radiotracer uptake values in the myocardium to calculate a cardiac metabolic activity (CMA).
A total of 56 patients completed the initial six-month therapy regimen, with two patients having died and one who discontinued participation. In 47 patients allocated to the response group, the median cardiac metabolic activity dropped from 203.3 to 1 (p < 0.001), the group found. In the 11 initial nonresponders who received methotrexate or a second round of prednisolone for six months, no additional significant reduction in cardiac metabolic activity values were observed, the researchers noted.
"This study is the first to prospectively examine the effectiveness of immunosuppressive therapy by quantitatively evaluating FDG accumulation using CMA in patients with cardiac sarcoidosis," the authors wrote.
The group did acknowledge that the study had a limitation, namely that while methotrexate is expected to be a complementary and alternative option to prednisolone, Morimoto and colleagues did not compare the regimens in patients unresponsive to initial therapy.
"Future multicenter studies involving a larger number of cases are needed to further evaluate the efficacy of methotrexate," the researchers concluded.
The full article is available here.