Tuesday, November 30 | 9:30 a.m.-10:30 a.m. | SSCH04-4 | Room TBA
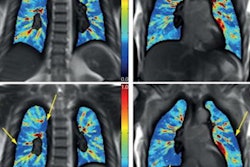
It's important to include vaping history when treating patients presenting with acute lung injury (ALI) -- especially if they are young and appear healthy, according to research to be presented on Tuesday.Dr. Seth Kligerman of the University of California, San Diego and colleagues found there are a wide range of findings on CT scans of people with electronic cigarette or vaping-associated lung injury (EVALI), and some are less typical.
"Some patients [demonstrate] CT findings less commonly reported in other causes of ALI, including superimposed upper lobe predominant centrilobular nodules and peribronchovascular sparing," Kligerman's team wrote in the study abstract.
The group assessed the CT scans of 160 patients (mean age, 28) who had an EVALI diagnosis, noting the frequency of vaping, substance used, and the severity of the injury. Of the study cohort, 48.1% reported vaping THC, 9.4% reported vaping nicotine, and 42.5% reported vaping both.
The investigators defined the following typical CT finding patterns for their assessment:
- Parenchymal organizing pneumonia pattern: regional or diffuse ground-glass opacities (with or without consolidation) without centrilobular nodules
- Airway-centered parenchymal organizing pneumonia: diffuse centrilobular nodules with little or no ground-glass opacities
- Mixed parenchymal organizing pneumonia: a combination of first two patterns
- Diffuse alveolar damage
- Acute eosinophilic pneumonia-like
- Pulmonary hemorrhage
Most patients (97.5%) manifested at least one of these common CT patterns, with diffuse or lower lobe ground-glass opacities with subpleural (78.1%), lobular (59.4%), or peribronchovascular sparing (40%) being the top three. But Kligerman's group also noted parenchymal, airway-centered, and mixed-organizing pneumonia patterns (55.6%, 8.8%, and 20%).
"EVALI typically causes an organizing pneumonia pattern but exists on a spectrum of acute lung injury," they concluded.