Measuring arterial plaque with cardiac CT in addition to established tests for heart disease can help predict which patients may suffer life-threatening events, according to a presentation at the virtual 2021 Society of Cardiovascular Computed Tomography (SCCT) meeting.
The researchers analyzed data on patients with severe coronary artery disease (CAD) who had already undergone cardiac CT angiography (CCTA) and SPECT tests. When they added scores that measured coronary plaque, they found they could better predict patients' risk for events such as stroke or death.
"Our results suggest that in high-risk patients with suspected CAD, plaque burden adds incremental prognostic value over established measures in predicting incident cardiovascular outcomes," said SCCT presenter Dr. Ahmed Ibrahim Ahmed of Houston Methodist DeBakey Heart and Vascular Center in Houston, Texas.
CCTA and SPECT myocardial perfusion imaging are established tests for evaluating ischemia and stenosis in patients with heart disease. CCTA-derived measures of plaque, such as segment involvement score (SIS), or the percentage of plaques in affected arteries, also independently predict severe events.
However, most studies have focused on diagnostic accuracy of the imaging tests without accounting for coronary atherosclerotic burden, according to Ahmed and colleagues.
In this study, the researchers aimed to assess the incremental prognostic value of plaque burden in a high-risk CAD group of patients who had undergone both CCTA anatomic assessment and SPECT physiologic assessment tests.
The researchers included 956 patients (54% men) with suspected CAD who had undergone CCTA and SPECT myocardial imaging at Houston Methodist between January 2016 and June 2020. The SIS was defined as the sum of segments with plaque, irrespective of the degree of stenosis, using an 18-segment coronary artery model. Patients were followed for major adverse cardiovascular events.
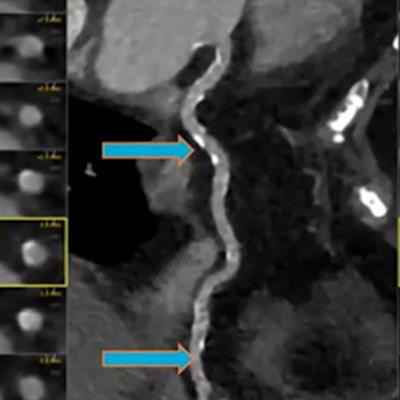
 A 56-year-old patient with a clinical history of hypertension, diabetes, and dyslipidemia. Cardiac CT angiography showed obstructive stenosis. The segment involvement score was 11. Image courtesy of Dr. Ahmed Ibrahim Ahmed.
A 56-year-old patient with a clinical history of hypertension, diabetes, and dyslipidemia. Cardiac CT angiography showed obstructive stenosis. The segment involvement score was 11. Image courtesy of Dr. Ahmed Ibrahim Ahmed.After a median follow-up of 31 months, 102 patients experienced a major event. An analysis showed SIS significantly predicted outcomes and improved risk discrimination in patients with CCTA obstructive stenosis (hazard ratio, 1.15) and SPECT ischemia (hazard ratio, 1.14). The CCTA hazard ratio was statistically significant, while the SPECT one was not.
"Plaque burden was associated with primary outcome, with hazard ratios showing each additional [SIS] segment added 15% increase in risk for incident events," Ahmed said.
The fact that patients had received both CCTA and SPECT myocardial perfusion imaging for clinical indications limits generalizing the findings in patients with similar characteristics, Ahmed noted.
Ultimately, the results suggest that in high-risk patients with suspected CAD, plaque burden adds incremental prognostic value over established measures in predicting incident cardiovascular outcomes, Ahmed et al concluded.