The novel coronavirus disease (COVID-19) is characterized by CT findings that match features of other pneumonia-causing viruses. But radiologists from the U.S. and China demonstrated that they are well-equipped to differentiate COVID-19 from these other viruses in a new study, published online March 10 in Radiology.
Nucleic acid testing with reverse transcription polymerase chain reaction (RT-PCR) remains the principal method for confirming COVID-19, but the diagnostic test is limited by its long processing time and low sensitivity for early disease detection. Recent studies have shown chest CT to be much more sensitive than RT-PCR at detecting COVID-19 in its early stages, albeit with low specificity, suggesting that CT has the potential to bolster DNA testing.
"This low specificity [for CT] may stem from the fact that it is difficult to distinguish COVID-19 findings from findings of other disease on chest CT. ... For example, influenza and COVID-19 both demonstrate ground-glass opacity and consolidation on chest CT," wrote a team of researchers led by Dr. Harrison Bai from Rhode Island Hospital.
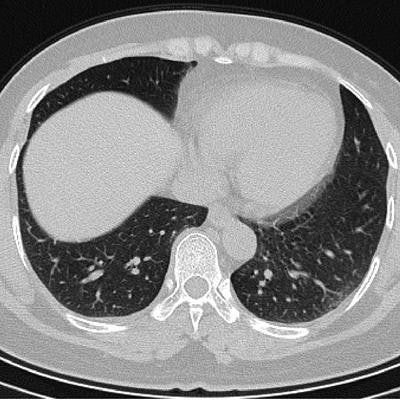
 CT images of a patient with pneumonia misdiagnosed with COVID-19 (above) and a patient with COVID-19 misdiagnosed with non-COVID-19 pneumonia (below). All images courtesy of the RSNA.
CT images of a patient with pneumonia misdiagnosed with COVID-19 (above) and a patient with COVID-19 misdiagnosed with non-COVID-19 pneumonia (below). All images courtesy of the RSNA.In the current study, Bai and colleagues evaluated the ability of radiologists to distinguish COVID-19 from other viruses on CT without knowledge of the patients' RT-PCR results or clinical information.
Three radiologists from China examined the chest CT scans of 424 patients with pneumonia caused by either COVID-19 or a different virus. They demonstrated relatively high accuracy and specificity and moderate sensitivity for detecting COVID-19. The researchers subsequently selected a random subset of 58 age-matched cases for examination by the three radiologists from China and four additional radiologists from the U.S.
On average, the radiologists proved capable of distinguishing COVID‑19 from other common viral pneumonia on chest CT with an accuracy of 82.1%, a specificity of 83.7%, and a sensitivity of 80.4%.
Despite minimal training specific to diagnosing COVID-19, the radiologists showed that they were capable of distinguishing COVID-19 from other etiology of pneumonia on chest CT with high specificity, the authors noted.
"This suggests that there is potential that if the differential diagnosis is between COVID-19 and non-COVID-19 pneumonia, a negative diagnosis of COVID-19 by radiologists on chest CT may be good enough to exclude patients from having the disease with fairly good certainty," they wrote.
The researchers also listed several CT patterns that were much more common in patients with COVID-19 than in those without the disease: ground-glass opacity, peripheral distribution, vascular thickening, fine reticular opacity, and reverse halo sign.
| CT findings for COVID-19 vs. non-COVID-19 pneumonia | ||
| Non-COVID-19 | COVID-19 | |
| Ground-glass opacity | 68% | 91% |
| Peripheral distribution | 57% | 80% |
| Vascular thickening | 22% | 59% |
| Fine reticular opacity | 22% | 56% |
| Reverse halo sign | 1% | 5% |
"It is recommended that individuals with signs of pneumonia on chest CT be quarantined while RT-PCR testing is performed in conjunction with a thorough medical evaluation including travel history and disease contacts in order to make an accurate COVID-19 diagnosis and prevent disease spread," the authors concluded.



















