Researchers from China and the U.S. have succeeded in producing ultralow-dose coronary CT angiography (CCTA) exams in a wide range of patients using iterative reconstruction. In the process, they've helped redefine low-dose CCTA to mean far less than 1 mSv in all patients, according to study results published in JACC Cardiovascular Imaging.
In the study, 60 individuals with suspected coronary artery disease underwent conventional invasive angiography and dual-source CCTA twice: once with conventional radiation dose settings and once again at half the dose reconstructed with iterative reconstruction (IR). The researchers found that image quality scores and diagnostic accuracy did not suffer when low-dose settings were combined with a commercially available iterative reconstruction scheme.
Compared with angiography as the gold standard, CCTA's per-segment sensitivity for diagnosing coronary stenosis of at least 50% was 88.5% at the regular radiation dose with filtered back projection (FBP) and 84.2% using half the dose and iterative reconstruction. Specificity was actually higher at the lower dose, with 92.1% for FBP and 93.4% for iterative reconstruction.
What's more, the median dose-length product (DLP) was 52% lower for the IR protocol, at a mean 52 mGy-cm (0.76 mSv) for IR, compared with 109 mGy-cm (1.52 mSv) for the standard-dose protocol (JACC Cardiovasc Imaging, October 2013).
"Using the iterative reconstruction method, we can use half traditional mAs to perform CCTA without sacrificing image quality or diagnostic accuracy ... and the radiation dose could be reduced by more than 50%," study co-author Dr. Bin Lu from Fuwai Hospital in Beijing wrote in an email to AuntMinnie.com.
Twice as nice
At least two things are new about this study, co-author Dr. U. Joseph Schoepf from the Medical University of South Carolina told AuntMinnie.com in an interview.
"This is one of the few examples in the literature where patients were actually scanned twice in order to exactly figure out what a certain variable does in terms of image quality," he said. "If you scan patients twice there is no uncertainty," as there is with two separate cohorts, "where you have too many confounding variables to determine if your intervention caused the result or if it's just bias because of the different composition of the groups. So I think scanning the same patient twice is a much cleaner solution."
Not long ago it would have been problematic to scan patients twice owing to the vastly higher radiation doses and greater amounts of contrast material used in CT, he said. But these days, advances in CT techniques have made it "perfectly ethical" to subject a patient to two CCTA scans, especially considering that the total dose with both acquisitions is 2.2 mSv. And it's really the combination of advanced techniques that paved the way for very low doses, he added.
For the current study, lead author Dr. Wei-Hua Yin and colleagues utilized quite an array of techniques. A day or two before conventional angiography, patients underwent CCTA scanning on a second-generation dual-source scanner (Somatom Definition Flash, Siemens Healthcare). Settings included 2 x 64 x 0.6-mm collimation and tube current modulation (CARE Dose4D, Siemens) applied by default. Automated bolus tracking with 50 mL to 60 mL of undiluted contrast agent was followed by a saline chaser.
The two scans were acquired within minutes of each other, and except for the tube current product, all scan parameters and contrast dosing were kept constant. For patients with a body mass index (BMI) > 25 kg/m2, 120-kV tube potential with a 320-mAs tube current-time product was used; for BMI between 20 and 25 kg/m2, 100 kV with 370 mAs was used; and for BMI < 20 kg/m2, 80 kV with 400 mAs was used. For the scans acquired with iterative reconstruction in mind, tube current-time products were reduced by 50% -- that is, to 160 mAs with 120 kV, 186 mAs with 100 kV, and 200 mAs with 80 kV, the group noted.
The study population consisted of patients with a wide range of body sizes, including two with BMI < 20 kg/m2, 24 patients with BMI between 20 and 25 kg/m2, and 34 patients with BMI > 25 kg/m2.
All images were reconstructed using 0.75-mm section thickness, a 0.5-mm reconstruction increment, and a 200-mm field-of-view. The FBP images used a medium-smooth tissue convolution algorithm (B26f), with the corresponding I26f kernel used for iterative reconstruction. The series were also reconstructed using the higher-resolution B46f and I46f algorithms, the authors wrote.
The IR images were reconstructed using a second-generation reconstruction scheme (sinogram-affirmed iterative reconstruction [SAFIRE], Siemens) that operates primarily in the raw data space, using initial voxel attenuation coefficients to predict projection data. The projection data are then compared with actual data, the study team explained.
Within a day or two of CCTA, the group performed coronary angiography according to the standard Judkins technique.
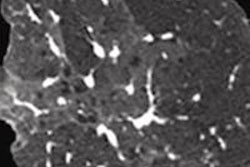
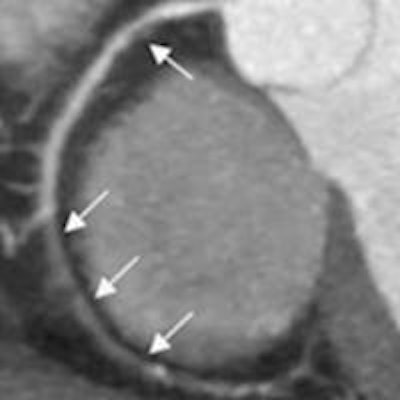
 61-year-old woman (body weight, 65 kg; heart rate, 57 beats/min) with suspected coronary artery disease underwent two coronary CTA acquisitions using prospectively electrocardiogram-triggered high-pitch spiral technique. Multiple high-grade stenosis (local nearly occlusive) and noncalcified plaque of the right coronary artery are shown on maximum-intensity projection in both FBP (left) and IR (middle) series. The lesion was confirmed by subsequent coronary catheter angiography (right). The dose-length products were 62 and 31 mGy-cm for the FBP and IR protocols, respectively. Image courtesy of Dr. Bin Lu.
61-year-old woman (body weight, 65 kg; heart rate, 57 beats/min) with suspected coronary artery disease underwent two coronary CTA acquisitions using prospectively electrocardiogram-triggered high-pitch spiral technique. Multiple high-grade stenosis (local nearly occlusive) and noncalcified plaque of the right coronary artery are shown on maximum-intensity projection in both FBP (left) and IR (middle) series. The lesion was confirmed by subsequent coronary catheter angiography (right). The dose-length products were 62 and 31 mGy-cm for the FBP and IR protocols, respectively. Image courtesy of Dr. Bin Lu.According to the results, the per-segment sensitivity for diagnosing 50% or greater coronary artery stenosis was 88.5% with FBP and 84.2% with iterative reconstruction. Specificity was 92.1% with FBP and 93.4% with iterative reconstruction.
With FBP, the area under the receiver operator characteristics (ROC) curve was 0.903 (95% confidence interval [CI]: 0.881-0.922), compared with 0.888 (95% CI: 0.864-0.909) for iterative reconstruction on a per-segment level.
Compared with FBP, the iterative reconstruction series showed no statistically significant differences (p > 0.05) in subjective image quality analyses, despite a median dose-length product that was 52% lower with the IR protocol than the FBP protocol. Median dose-length product was 109 mGy-cm for the FBP protocol and 52 mGy-cm for iterative reconstruction.
"Our direct, intraindividual head-to-head comparison in the same patient population shows that compared with a routine radiation dose FBP protocol, a 50% reduced radiation dose image acquisition using IR preserves image quality and, more importantly, diagnostic accuracy at coronary CTA," the authors wrote. "These findings illustrate the potential of substantial radiation dose reduction across the population for coronary CTA studies, enabled by a reduced tube current-time product when iteratively reconstructed, without jeopardizing the diagnostic yield of the examination."
Ethical considerations
The study couldn't have been performed without advanced acquisition techniques for ethical reasons, the group noted. The mean total contrast media volume of approximately 125 mL and the median dose-length product of about 161 mGy-cm received from the two CT scans were "very well within the limits of routine clinical applications, as well as of common research settings," Yin and colleagues wrote.
Larger multicenter trials are needed to validate the results, they noted.
"In this context, it is also of consideration that we investigated an Asian population, who generally tend to have leaner body types than average patients in Western societies," the authors wrote.
"Here we're looking at a total radiation dose of 2.2 mSv at most per patient from both of the examinations, and also the amount of contrast media that people receive is very well within the limits of a clinically indicated CT study that's done every day," Schoepf said. "So the improvements in technology that people have seen actually do give us the opportunity where patients serve as their own control and are investigated twice."