A novel color-coded fecal-tagging method significantly cut interpretation time for reduced-prep virtual colonoscopy (VC or CT colonography), easing a task that can be tiring and time-consuming for radiologists.
According to researchers from Korea, the color-coding method was not only popular with readers, it pared nearly three minutes from mean interpretation times without any loss of sensitivity. Their research was published in the September issue of Radiology (Vol. 248:3, pp. 1018-1027).
Virtual colonoscopy performed without cathartic bowel cleansing offers clear advantages for patients, who find laxative preparations burdensome and may even skip screening to avoid the discomfort. On the other hand, reduced-prep VC has its own limitations, noted study authors Dr. Seong Ho Park and colleagues from University of Ulsan College of Medicine, Asan Medical Center; and the National Cancer Center, both in Seoul.
"One of the greatest concerns is that it does not work well with primary three-dimensional (3D) interpretation," they wrote. "On a typical monochromatic volume-rendered 3D endoluminal view, a polyp cannot be distinguished from polyplike tagged stool. Therefore, primary 3D interpretation of CT colonographic images obtained with reduced cathartic preparation would require a large number of two-dimensional (2D) correlations or references to translucency maps for confirmation of numerous luminal protrusions," making interpretation more cumbersome.
In an effort to facilitate the reading of 3D datasets in reduced-prep VC, the authors evaluated a new technique for discriminative color coding of tagged stool during endoluminal fly-through, testing its efficacy in primary 3D reading of moderate-prep VC. The method is designed to take advantage of 3D's strengths, including better polyp conspicuity and a less fatiguing search pattern for many readers, the authors wrote.
A total of 30 patients (16 women and 14 men; mean age, 58.3) were prepared with moderate cathartic solution (20 mg bisacodyl, three doses of 200 mL of a 5% barium sulfate preparation). Thirteen of the 30 patients were asymptomatic screening subjects, while the remainder had reported a change in bowel habits or other conditions suggestive of an elevated risk of colorectal polyps and cancer.
Following automated insufflation of the colon with CO2 (ProtoCO2L, Bracco Diagnostics, Princeton, NJ), supine and prone scans were acquired using a 16-slice CT scanner (Somatom Sensation 16, Siemens Healthcare, Erlangen, Germany) with collimation of 0.75 mm, 1-mm reconstructed section thickness, 0.7-mm reconstruction interval, 120 kV, and 30 mAs.
"For selective discriminative color coding of tagged stool during 3D endoluminal fly-through CT, we developed a technique of volume rendering with attenuation-dependent color enhancement," the authors explained. "The technique is a modification of the commonly used perspective ray-casting method in which multiple rays of light are cast from an imaginary light source to the target volumetric CT dataset. With the ray-casting method, attenuation values of the data points along the path of each ray are checked, and then opacities and colors are assigned to those data points according to a predefined opacity and color for each attenuation value."
The technique creates an endoluminal image of the colon from the partial-volume layer, which is based on data points between the bowel wall and the luminal air regions. The algorithm then checks the attenuation of data points along each ray path beyond the point of 95% opacity from the light source, representing the opaque bowel wall. If the attenuation changes by more than 200 HU within 2 mm of these opaque data points, indicating tagged fecal material adjacent to the wall, the color of this region is changed to white.
"The threshold value of 200 HU was chosen in consideration [of] previous studies about subtraction of tagged stool and polyp attenuation on CT colonographic images to eliminate the possibility of coding a true colonic polyp as white," they noted.
To evaluate the results of the method on readers, two experienced radiologists reviewed the 3D CT colonography (CTC) datasets randomly with and without the color-coding feature in sessions separated by a month's time. They used 2D correlation as needed, for example to interpret lesions completely covered by tagged stool. All findings were correlated with optical colonoscopy performed within two months of VC.
After excluding patients with incomplete colonoscopy, 27 datasets were included in the study results. A total of 47 lesions 6 mm or larger were detected in 16 patients at colonoscopy. Colonic distension was rated good to excellent in six colonic regions, with the exception of a collapsed segment in one patient. Average fecal tagging scores ranged from 73.1% in the rectum to 84.7% in the transverse colon, the authors noted. Both readers preferred color coding, which reduced interpretation times by 3 minutes for reader 1 (p = 0.002) and 2.5 minutes for reader 2 (p = 0.009).
"The number of 2D correlations during the primary 3D review decreased significantly when the discriminative color coding of tagged stool was used: A mean of 9 ± 6.6 was observed with the discriminative color coding versus a mean of 52.9 ± 45.7 without the discriminative color coding for reader 1 (p < 0.001), and a mean of 14.5 ± 7.9 was observed with the discriminative color coding versus a mean of 57.1 ± 37.8 without the discriminative color coding for reader 2 (p < 0.001)," Park and colleagues reported.
Both with and without use of the color-coding feature, sensitivity for lesions 6 mm and larger remained at 96% (24 of 25; 95% confidence interval: 78.9%, < 100%; p ≥ 0.99).
"Our results clearly show that selective discriminative color coding of tagged stool by using this technique facilitated the primary 3D interpretation of CT colonographic images that were obtained with moderate cathartic preparation, as it allowed an easier and more time-efficient review of CT images while maintaining diagnostic accuracy," the group concluded.
The color-coding technique permitted the easy dismissal of tagged stool, while the readers were able to set aside completely tagged areas for 2D correlation, significantly reducing the number of "repetitive" 2D correlations required during the fly-though.
"Compared with primary 2D review of the entire ... dataset, which requires tracing of the complex colonic outline on each 2D image, the supplementary 2D search is an easier task," they explained. "The reader moves from one relatively small region of interest to another to look for submerged polyps rather than [tracing] a large area of complex colonic contour."
 |
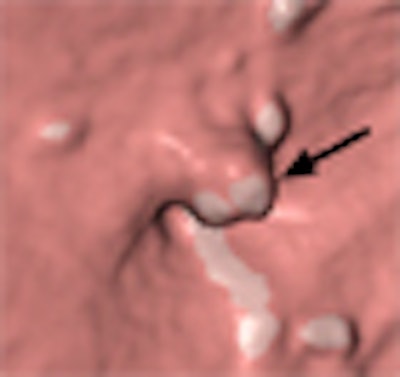
| Luminal protrusions with partially white areas after application of discriminative color-coding technique for tagged stool (arrow) in a 6-mm-diameter partially tagged polypoid stool in a 78-year-old woman. Image republished with permission of the Radiological Society of North America; from Park SH, Lee SS, Kim JK, et al. Volume rendering with color coding of tagged stool during endoluminal fly-through CT colonography: Effect on reading efficiency. Radiology. 2008;248(3):1018-1027. |
Only "eye tracing" of the white-gray tagged regions is needed for the color-coded approach, compared to the simultaneous tracing of both the luminal air-colonic wall and the tagged stool required for 2D review of the entire dataset, the group noted.
"The improved subjective ease in interpretation with the color-coding tool may be important with respect to eye strain, motivation, and longevity of reading sessions," they wrote.
 |
| Supplementary 2D review of colonic surfaces covered by tagged stool in 78-year-old woman. Three-dimensional endoluminal view of rectum after application of discriminative color-coding technique clearly distinguishes large amount of white-tagged stool (arrowheads) from red-to-brown colonic wall. A 6-mm-diameter polyp that is completely buried under the tagged stool (dotted elliptical line indicating location of buried polyp) cannot be found on 3D view. Image republished with permission of the Radiological Society of North America; from Park SH, Lee SS, Kim JK, et al. Volume rendering with color coding of tagged stool during endoluminal fly-through CT colonography: Effect on reading efficiency. Radiology. 2008;248(3):1018-1027. |
Among the limitations, color coding would probably be less effective when large amounts of tagged stool are present, the authors stated, because more supplementary 2D review would be needed. Also, the technique may not work uniformly across different CTC systems, pending further study. Finally, they noted that most of the clinically important lesions in the small cohort of patients were 10 mm or larger, facilitating their detection.
By Eric Barnes
AuntMinnie.com staff writer
September 5, 2008
Related Reading
Automated polyp measurement supports risk assessment, August 26, 2008
Image tools cut false positives in unprepped VC, August 4, 2008
Higher VC laxative dose burdens patients, doesn't improve reads, July 16, 2008
VC CAD finds polyps in prepped or unprepped patients, May 6, 2008
Minimal-prep VC may miss more flat lesions, April 17, 2008
Copyright © 2008 AuntMinnie.com

















