This article continues our series of white papers on radiologic patient positioning techniques. Appearing each month on AuntMinnie.com, the series explores each of the major modalities. If you'd like to comment on or contribute to this series, please e-mail [email protected].
The anteroposterior (AP) radiograph taken with the patient in a supine position is the basis of the majority of plain-film examinations of the abdomen. The abdominal film obtained with the patient in an erect position is ordered routinely, but rarely adds significant diagnostic information. However, an upright-position film may be helpful in patients with suspected bowel obstruction, as well as to assess the air-fluid levels in the distended bowel.
This information can also be obtained on a film of the abdomen taken with the patient in the lateral decubitus position. An AP supine projection is often called a flat plate or KUB (because it includes the kidneys, ureter, and bladder).
The following are the main reasons abdominal films are requested:
- Bowel obstruction -- abnormal gas pattern .
- Free intraperitoneal air (pneumoperitoneum).
- Free intraperitoneal fluid (ascites).
- Abnormal size or contour of organs.
- Abnormal masses.
- Calculi or other abnormal intra-abdominal calcifications.
- Radiopaque foreign bodies.
- As a preliminary radiograph before performing a gastrointestinal series with contrast, an intravenous pyelogram (IVP), or other radiological procedures.
- To assess the positions of intra-abdominal tubes and catheters.
Preliminary bowel preparation
Preliminary bowel preparation in nonacute patients is administered with a combination of laxatives, enemas, and controlled diet. Preparation is important if the patient will be undergoing contrast examination of the gastrointestinal tract or an IVP.
In all other cases, the decision regarding whether or not a patient undergoes preliminary bowel preparation is determined by the requesting physician. Bowel preparation should not be administered to patients suspected of having bowel obstruction, visceral perforations, or abdominal trauma, or to an acutely ill patient.
Patient preparation
Ask the patient to remove all clothing and put on a hospital gown. If the patient cannot do so, remove any opaque objects in the clothing that can cause artifacts in the area to be x-rayed. Use gonadal shielding on males; the upper edge of the shield should not be above the pubic symphysis. In female patients, an ovarian shield can obscure pelvic anatomy, so one should not be used unless the physician requests it.
Position of the patient
- If a supine-position radiograph is ordered, placing a support under the knee helps to relieve the strain on the patient while they are in the supine position.
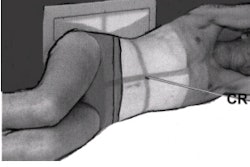
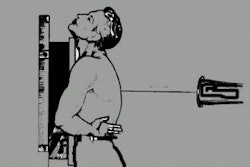
- For upright-position radiograph, the patient’s back should be against the grid device, legs slightly spread, with body weight distributed equally on both feet.
- In both positions, the midsagittal plane of the body should be centered to the midline of the grid device.
- There should be no rotation of the shoulder and pelvis.
- Place the patient's arms at the sides and away from the body.
 Standard AP supine and upright abdominal patient position. Image courtesy of Dr. Naveed Ahmad.
Standard AP supine and upright abdominal patient position. Image courtesy of Dr. Naveed Ahmad.Position of abdomen
- The most commonly used abdominal landmark is the iliac crest, which corresponds to the level of the mid-abdomen and is at the L4-L5 vertebral inter-space level. The iliac crest is at the uppermost position of the curved border of the ilium.
- For the supine position, the cassette or image receptor (IR) is centered to the iliac crest and the lower abdomen is generally included on the lower margin of the cassette.
- For the upright position, the cassette is centered 2 inches (5 cm) above the level of the iliac crest, or high enough to include the diaphragm.
- Maximal relaxation of the abdominal musculature is important in reducing film artifact caused by motion. Relaxation of the abdominal musculature is facilitated by supporting and slightly flexing the patient’s knees.
- Two radiographs may be needed if the patient is very tall.
- The exposure is made during expiration and should begin 1-2 seconds after respiration is suspended. Ask the patient to take a deep breath, exhale completely, and then hold the position while not inhaling. This moves the diaphragm to a superior position that results in better visualization of the abdominal viscera.
Film holder placement
A 14 x 17-inch (35 x 43-cm) film or IR should be positioned lengthwise, with its lower edge at the symphysis pubis. Crosswise cassette placement is appropriate if the patient is very large.
Central ray
- For a supine-position radiograph, the central ray (CR) should be perpendicular to the cassette at the level of iliac crests.
- For an upright-position film, the CR should be horizontal and 2 inches (5 cm) above the level of the iliac crests and should include the diaphragm.
Collimation
For abdominal radiographs of small patients, some side collimation of the side borders is possible -- if it does not cut off abdominal anatomy. For adults, collimation on the top and bottom should be adjusted to the margins of the film holder, allowing for divergence of the x-ray beam.
Imaging technique
- Film or IR size: 14 x 17 inches (35 x 43 cm) lengthwise
- Moving or stationary grid
- 70-80 kVp range
- mAs 30
- Sk 396
- cm 21
 AP abdominal image showing important evaluation criteria. Image courtesy of Dr. Naveed Ahmad.
AP abdominal image showing important evaluation criteria. Image courtesy of Dr. Naveed Ahmad.Evaluation criteria for a good AP projection
- The image should include the area from the upper border of the pubic symphysis to the diaphragm.
- Proper alignment -- the vertebral column should be in the midline position. Ribs, pelvis, and hips should be equidistant to the edge of the radiograph.
- No rotation -- spinous processes in the center of the vertebral column and symmetric ilial wings
- No motion -- ribs and gas bubble margins should appear sharp. The diaphragm should appear sharp in an upright film.
- Soft tissues visualization -- correctly exposed abdominal radiographs on an average-size patient should faintly visualize the lower liver margin, kidneys, the lateral borders of psoas muscles, and transverse processes of lumbar vertebrae.
- Appropriate markers should be placed indicating either upright or supine position.
AuntMinnie.com contributing writer
January 16, 2002
Copyright © 2002 AuntMinnie.com