Testicular Imaging
Technique
The agent used for testicular imaging is Technetium-pertechnetate 15 mCi IV (minimum dose 5 mCi). Potassium-perchlorate (5 mg/kg) is given immediately before the exam to block thyroid uptake of the tracer. Flow images are obtained, and immediately followed by static and pinhole images. A marker view indicating the symptomatic side should always be obtained.
The blood supply to the testes is via the testicular, cremasteric, and deferential arteries. The testicular artery supplies the majority of the blood flow. The 3 vessels run with the spermatic cord and anastamose in close proximity to the testes. The cremasteric artery also supplies the scrotal wall. Blood supply to the scrotum is via the branches of the pudendal artery. The internal pudendal and the superficial and deep external pudendal arteries supply the scrotum and penis. These vessels are external to the spermatic cord and are not affected by torsion.
Testicular Torsion
Acute scrotal pain and swelling may be due to a variety of conditions including torsion, epididymitis, torsion of the appendix testes, orchitis, or a strangulated hernia. Testicular torsion is a surgical emergency. Testicular salvage rates depend on the duration of ischemia, with a nearly 100% salvage rate within the first 6 hours. Beyond this point, the salvage rate drops quickly and by 24 hours the testicle is essentially infarcted.
Although torsion can occur at any age, the peak incidence is in adolescence, with a smaller peak in pediatric patients between 0 and 3 years.
Testicular ultrasound has become a very convenient way to evaluate the testicles for perfusion, but it may be difficult to detect normal flow in pediatric patients. In these instances, scintigraphy is a reasonable alternative to evaluate the patient.
Normally, the vessels supplying the scrotum are ill-defined and the scrotum and its contents blur into a homogeneous area of tracer accumulation similar in intensity to the thigh. Scintigraphy has a sensitivity of 90% in the evaluation of testicular torsion.
The scintigraphic findings in torsion depend on the duration of torsion and they are typically divided into early, mid, and late phases.
Early phase (Acute torsion)
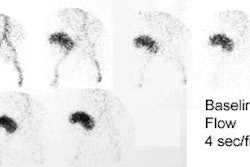
Blood flow may appear normal or decreased to absent on the involved side. Blood flow is never increased during this stage. A "nubbin" sign may be seen as a bump of activity extending medially from the iliac artery, denoting reactive increase in blood flow in the spermatic cord with abrupt termination. Static images show decreased tracer accumulation within the involved testicle without evidence of the surrounding halo of increased activity noted on later phases.
Mid Phase
After 6 to 18 hours there is reactive hyperemia in the region supplied by the pudendal arteries. The flow portion of the study shows increased blood flow to the dartos, and early static images show a halo of mildly increased activity around a centrally cold testicle. This halo gradually disappears on subsequent images.
Late Phase
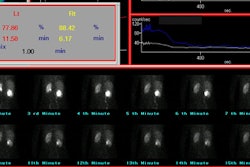
By this time, irreversible testicular infarction has occurred. There is marked increased flow to the dartos, with a persistent halo of increased activity around a cold center on static images. This is a sign of non-viability of the testicle with surrounding hyperemia within the pudendal vasculature.
Late torsion: The patient presented after 3 days of left scrotal pain. A halo of increased tracer activity can be seen about the left testicle with a cold center. |
|

Spontaneous detorsion may appear normal, or may show a slight, diffuse increased scrotal activity if the scan is obtained shortly after detorsion has occurred. An intact blood supply to the testicle obviates only the need for emergent surgery. If the patients history is typical of intermittent torsion, elective orchiopexy may be indicated.
Torsion of the Testicular Appendages
Torsion of the appendix testis or epididymis will result in symptoms of acute scrotal pain and classically produce a focal area of increased blood flow and blood pool activity, probably secondary to reactive hyperemia around the torsed appendage. A more common scintigraphic pattern is that of mild generalized increased blood flow and pool activity which may be indistinguishable from that seen with epididymitis.
Acute Epididymitis
There is marked increased flow and blood pool activity which may be focal or diffuse in the involved scrotum. Increased activity in the epididymis may occasionally resemble the halo of late phase torsion, but the rim will be incomplete or asymmetric. Epididymitis in infants and young children may be secondary to an underlying anatomic abnormality, such as an ectopic ureter, and warrants further investigation.
Abscess
Scans show a cold area surrounded by a rim of increased activity which is indistinguishable from late phase torsion.
Scrotal Trauma
Mild traumatic changes may appear as slightly to moderately increased diffuse tracer accumulation. An intratesticular or intrascrotal hematoma may appear as a cold lesion with or without a surrounding halo of increased activity, indistinguishable from testicular torsion.
Hydrocele
Scans show a horseshoe or half-moon shaped area of photopenia surrounding the testicle. A hydrocele should be readily identified on physical examination of the patient.
REFERENCES:
(1) Semin Nucl Med 1990; Lutzker LG, Zuckier LS. Testicular scanning and other
applications of radionuclide imaging of the genital tract. 20(2):159-88. Review.