This article originally appeared in the American Journal of Roentgenology, written by Dr. Howard Forman, associate editor of health policy for the American Roentgen Ray Society (ARRS).

The State Children's Health Insurance Program (SCHIP) represents a model for political and policy success. This expansion of coverage to our nation's poorest children is important for a number of reasons. Those of you who provide imaging interpretation services to children are directly affected by this program. For those who are not directly affected, there are important lessons about future coverage changes and directions.
In writing this brief, I am hopeful that all readers will see the SCHIP as the rarest of legislation: bipartisan, tried and true, and considered a success, after almost 10 years of implementation. What is it about this program that has worked so well? Why is it a success? How might this provide a lesson on solving the problem of the uninsured?
The Balanced Budget Act of 1997 (BBA 1997) was one of the most dramatic acts in the history of Medicare. Hospitals were dramatically affected and physicians suffered from many of its effects.
This act included two major changes:
- The Sustainable Growth Rate legislation, which has resulted in ever-present legislatively imposed reductions in our reimbursement (which frequently get reversed on an annual basis by the U.S. Congress).
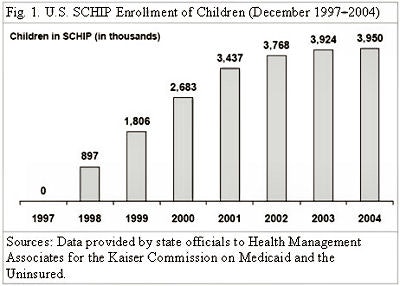
- A cap on the number of postgraduate trainees (residents) that are funded by Medicare. Also included was the SCHIP. By 1998, nearly 1 million children were enrolled, and at last count, almost 4 million children were insured by this program (see figure 1, below).
 |
This program is a federal-state partnership, much like Medicaid, but with key differences:
- It represented a real expansion in insurance options for poor children.
- It was a flexible limited entitlement (almost a block grant), thus maintaining the credibility of the bill ("balanced budget") for which it was included.
I believe these differences were the two main reasons why it was passed in a truly bipartisan manner.
The idea of transferring autonomy to the states, including budget autonomy, has been a platform of Republicans. True "block grants" are transfers of funds to the states from the federal government, with guidance, but otherwise no federal mandate on precisely how such funds can be used. The funding of the SCHIP is not quite a block grant, but it is a capped entitlement. These appeal to fiscal conservatives in giving states flexibility, while reducing federal obligations to some maximum. Democrats have persistently sought expansions in coverage for the uninsured, and this certainly meets that need.
In the case of the SCHIP, the results have been generally even better than expected, as few states have actually exhausted their SCHIP allotment. In the current fiscal year, Congress and the president have even gone so far (in the Deficit Reduction Act of 2005, passed into law in 2006) as to increase the authorized funding to enable all states to continue their plans, in full.
States are given a mandate to provide services, limited by the cap, to poor children who would not otherwise be eligible for Medicaid. Each state is allowed to expand the Medicaid program, create a new SCHIP or do some combination, in complying with the law. If the Medicaid program option is chosen, the enrollee must be offered the same benefit as other Medicaid beneficiaries. As with Medicaid, what has resulted is a tremendous variety in effort and success, but ultimately every state has complied with and tested new means of expanding the rolls of the insured. The SCHIP has reached a seeming plateau in the last few quarters. Four states had hit an enrollment cap as of December 2004: Florida, Utah, Idaho, and Montana.
The SCHIP is generally less than or equal to the generosity of the Medicaid program, so that in states with separate standalone SCHIP plans, there is generally a greater degree of cost-sharing and more limited coverage of services. On the other hand, this program is available to many more citizens than the Medicaid program, providing coverage to all children at or below 200% of the federal poverty level (FPL) who are not otherwise eligible for Medicaid.
Premiums are frequently charged, with 30 of the 38 separate programs requiring a premium that ranges from $5 to $100 per month (in the latter case, this premium applies to an entire family, an optional expansion of the program, allowed under the law).
When one thinks about the uninsured in America, we must remember that it is a very heterogeneous group. There are many who are too poor to afford insurance, in which case the Medicaid and SCHIP expansions reflect an appropriate policy solution. On the other hand, there are also many individuals who have sufficient means to afford health insurance but for whom the price is above their willingness (not ability) to pay. An appropriate policy solution for this group might lie in tax-related changes (see the September 2005 Policy Brief). Gaining the enrollment of all these individuals is as important to our practice as it is to making healthcare fair for all, thus, we can see room for both expansions of the SCHIP/Medicaid program and the use of our taxation system as models for reducing the number of uninsured in our country.
Ultimately, if one believes that there is no political possibility for a universal (nationalized) healthcare system in our country, we must consider how best to deal with the balance of fiscal prudence (with as low a tax burden as is feasible) with the ultimate desire to see nearly all of our population insured for necessary healthcare. The SCHIP is an interesting model. The program is up for reauthorization in 2007. As the uninsured problem in America has worsened, it is certain that the SCHIP will be renewed, but it may also be modified in ways that either expand or contract its mission. For those practitioners who already feel the pain of uninsured patients, this is an important moment. For those who dedicate much of their practice to pediatric imaging, it is all the more critical.
By Dr. Howard P. Forman
AuntMinnie.com contributing writer
July 10, 2006
Forman is an associate editor of health policy for the American Roentgen Ray Society (ARRS). This article originally appeared in the American Journal of Roentgenology (May 2006, Vol. 186:6). Reprinted by permission of the ARRS.
Related Reading
Offshoring, teleradiology, and the future of our specialty, March 20, 2006
M.B.A. education for physicians: cross-training options, January 25, 2006
Dual eligibles: Rarely mentioned, critically important, December 22, 2005
Government response to escalating imaging costs, December 12, 2005
Copyright © 2006 American Roentgen Ray Society