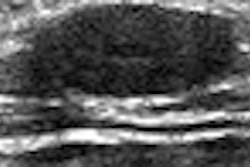
While it does offer fairly high specificity, bedside ultrasound for appendicitis (BUSA) by emergency physicians can't be relied upon to diagnose acute cases, according to researchers from the University of California - Irvine Medical Center in Orange, CA.
"We currently have insufficient evidence to rule out appendicitis by BUSA," according to Dr. Matthew Solley. He presented the team's research at the 2007 American Institute of Ultrasound in Medicine (AIUM) meeting in New York City.
Appendicitis is one of the most common abdominal surgical emergencies. Prior research into the role of ultrasound in diagnosing acute appendicitis has shown a broad range for sensitivity and specificity, Solley said.
To evaluate the accuracy of emergency physicians using BUSA, the researchers conducted a prospective study involving 132 patients. BUSA was performed by resident physicians or attending physicians, who had all participated in a one-hour didactic training on BUSA in an established emergency ultrasound program.
Patients were eligible for inclusion in the study if the attending physician suspected they had acute appendicitis. Patients were excluded if they were pregnant or unable to provide consent, according to Solley.
BUSA was then performed without interfering with routine workup, he said. Afterward, the study team followed up on the clinical course and outcome, including examining surgical pathology in patients who underwent appendectomy and telephone follow-up on patients discharged without appendectomy.
Of the 132 patients, five were lost during follow-up and one was excluded from the study. In the remaining 126 patients, BUSA yielded positive findings in 44 patients. Of these, 37 were true positives and seven were false positives.
Five of the false positives had a negative CT scan, were discharged home, and were asymptomatic at follow-up, Solley said. One of the other two had a negative radiology ultrasound and was found not to have appendicitis in the OR; the other patient was sent home and was asymptomatic at follow-up.
Negative BUSA findings were found in 82 cases: 62 were true negatives and 20 were false negatives. In one of the false-negative cases, CT was also negative but the patient still went to the OR and had their appendix removed. Among the other false-negative cases, eight had positive CT scans and went to the OR.
Two had a positive radiological ultrasound and went to the OR; one patient had a radiology ultrasound that was negative but a CT scan that was positive. Eight patients had no further imaging at all before going to the OR.
Overall sensitivity for BUSA was 65% and specificity was 90%. Positive predictive value was 84% and negative predictive value was 76%.
Solley acknowledged several limitations of the study, including the lack of blinding for sonographers, the variable experience of the sonographers, and the inclusion of patients without radiology imaging.
The evidence is insufficient to rule out appendicitis by BUSA, Solley concluded.
"Its high specificity (90%) might indicate there might be a chance to rule in some patients," he said. "With further training, we think this could eventually get on to be a useful (aid) in diagnosis."
By Erik L. Ridley
AuntMinnie.com staff writer
July 30, 2007
Related Reading
MR shows broad spectrum of findings in pregnant women with suspected appendicitis, July 3, 2007
Routine use of diagnostic CT not advised for suspected appendicitis, May 24, 2007
Patient and physician factors contribute to negative appendectomy, April 30, 2007
MRI accurately rules out appendicitis in pregnant patients, March 2, 2006
MDCT finds cause of acute abdomen more often with MPR, November 29, 2006
Copyright © 2007 AuntMinnie.com