Despite recent concerns over the use of CT in children, the modality is a good tool for diagnosing pediatric patients with clinical suspicions of pulmonary embolism (PE), according to an article in the September issue of the American Journal of Roentgenology.
In fact, clinicians from Children's Hospital Boston credit the use of CT angiography (CTA) exams for increased recognition of PE in children, as well as providing opportunities to assess for alternative diagnoses when the exam is negative.
A multidisciplinary research team led by pediatric radiologists Dr. Supika Kritsaneepaiboon and Dr. Edward Y. Lee analyzed four years of pediatric CTA exams to determine the prevalence and anatomic distribution of PE, along with the frequency and types of alternative diagnoses identified in children with clinically suspected but excluded PE. The current paper (AJR, September 2009, Vol. 193:3, pp. 888-894) is a follow-up to another study published in AJR in May (Vol. 192:5, pp. 1246-1252).
The initial study, which focused exclusively on the diagnosis of PE, included a cohort of 84 patients who underwent a total of 98 pulmonary CTA studies performed between July 2004 and August 2007. The second study expanded this cohort by 21 patients and 25 additional studies, performed between August 2007 and May 2008. The primary objective of the second study was to determine the frequency and types of alternative diagnoses that could be identified.
All of the children were clinically suspected of having PE. Their symptoms included shortness of breath, chest pain, increased oxygen requirements, tachycardia, hemoptysis, and pulmonary hypertension. The total cohort consisted of 36 boys and 69 girls, ranging in age from 2 months to 18 years. Eighty were outpatients and 43 were inpatients.
The majority of patients had only one examination. Additional studies were performed in cases where interval progression or resolution of PE after treatment needed to be determined.
CT parameters included weight-based kilovoltage settings, low-dose tube current, and a pitch equivalent of 1.0 to 1.5 using a combination of 16-, 32- and 64-slice MDCT scanners. Nonionic contrast media was administered by mechanical or hand injection.
The mean effective radiation dose was 9.9 mSv, with a range of 2.3 to 26 mSv. The authors attributed this wide variability in radiation dose to the use of three different MDCT scanners and differing pulmonary CTA protocols used over the 48-month time period.
The pulmonary CTA exams extended from the thoracic inlet to the level of the diaphragm and covered the entire lungs. Images for nonsedated patients were obtained in a single breath-hold at end-inspiration with the patient in the supine position. Images of sedated patients, primarily children younger than 5 years, were obtained at resting lung volume in the supine position.
For both studies, two experienced pediatric radiologists reviewed the CTA exams to determine the presence or absence of PE and for possible alternative diagnoses. The radiologists were blinded to prior imaging studies and all other clinical data, but they were aware that PE was suspected based on clinical signs and symptoms.
The exams were also evaluated and classified by specific criteria for image quality. Six exams performed after August 2007 were excluded, due to suboptimal image quality caused by suboptimal contrast enhancement or metallic artifacts obscuring pulmonary vessels.
PE diagnosis
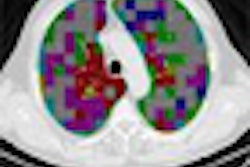
The radiologists confirmed a positive diagnosis of PE in a total of 21 studies (13 with the first study, eight with the second study) out of the 117 being evaluated, or a total of 17.9%. The diagnoses were made based on identification of a sharply delineated complete or partial pulmonary arterial filling defect present on at least two consecutive image sections located centrally in the vessel or with acute angles at its interface with the vessel wall.
The pulmonary emboli detected were lobar, segmental, and subsegmental. The PE was distributed bilaterally more often than unilaterally, but when unilateral, the right lung was involved more frequently than the left lung.
No isolated cases of subsegmental vessels were identified. In the majority of studies, these vessels were not optimally evaluated because of the lower rate of contrast visualization due to the small vessel size.
The authors reported that there was no correlation with prevalence of patient age. Because of these findings, they cautioned that radiologists should be aware that PE can occur in very young patients, including infants. There also was no correlation with the sex of the patient.
Thirty-nine (41%) of the remaining 96 studies, representing 38% of patients, were normal. Based on these data, the authors suggested that the normal rate among children with suspected PE in the general pediatric population could be between 31% and 51%.
Other diagnoses
The two most common alternative diagnoses in the remaining 57 studies were pneumonia and atelectasis. The radiologists diagnosed pneumonia in 22 cases, or 18.8% of the total, by identifying consolidation and patchy airspace opacifications. They diagnosed atelectasis, or a collapse of lung tissue, in another 22 cases.
Other diagnoses included malignancies, congenital heart disease, pulmonary hypertension, pericardial effusion, pulmonary nodules, and fat embolism. Seventeen patients showed pleural effusions that were associated with coexisting pneumonia, atelectasis, or rib fractures.
The authors attributed the diagnosis of pneumonia and atelectasis in 37.6% of the total number of cases to the fact that their clinical signs and symptoms are similar to those of PE. They suggested that if clinicians had used more stringent criteria for imaging patients with suspected PE in all years of the study, a larger percentage of patients may have had a positive diagnosis. In the fourth year of the study, 32% of 25 studies were positive, compared with 13.3% of the 98 studies performed in the first three years.
Pulmonary CTA exams are replacing ventilation-perfusion scintigraphy to diagnose PE, and they have replaced pulmonary angiography as the reference standard. The authors recommend that when a pulmonary CTA exam is performed, the interpreting radiologist should look for additional findings if the procedure is negative for PE.
By Cynthia E. Keen
AuntMinnie.com staff writer
August 25, 2009
Related Reading
Radiation dose and cancer risk in pediatric CTA exams, August 21, 2009
Coronary CTA with lower tube voltage reduces radiation exposure, April 27, 2009
Low tube current, modulation reduce pediatric CTA dose, May 21, 2008
Pediatric CT dose drops with breast shields plus tube modulation, February 26, 2008
Coronary CTA study aims for lowest dose, January 11, 2008
Copyright © 2009 AuntMinnie.com